Bae Soong June, Kim Jee Hung, Kim Min Ji, Kook Yoonwon, Baek Seung Ho, Kim Jung Hyun, Moon Sohyun, Lee Seung Eun, Jeong Joon, Cha Yoon Jin, Ahn Sung Gwe
Department of Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea.
Institute for Breast Cancer Precision Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
Breast Cancer Res. 2024 Dec 18;26(1):182. doi: 10.1186/s13058-024-01944-0.
Immunochemotherapy with pembrolizumab has been integrated into clinical practice as part of the standard-of-care for non-metastatic triple-negative breast cancer (TNBC) with high risk. We conducted a real-world study in TNBC patients treated with neoadjuvant chemotherapy to compare pathologic complete response (pCR) rates relative to stromal tumor-infiltrating lymphocytes (sTIL) across different regimens: non-carboplatin, carboplatin-, and pembrolizumab-chemotherapy.
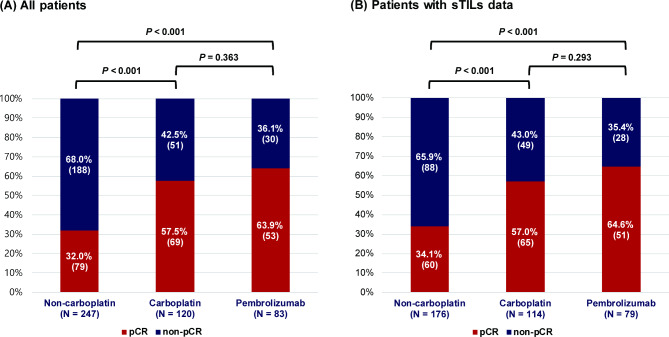
We analyzed a cohort of 450 patients with TNBC who underwent surgery following neoadjuvant chemotherapy between March 2007 and February 2024. Treatment groups included 247 non-carboplatin, 120 carboplatin, and 83 pembrolizumab-chemotherapy recipients. sTIL was evaluated in biopsied samples. Lymphocyte-predominant breast cancer (LPBC) was defined as tumors with high sTIL (≥ 50%).
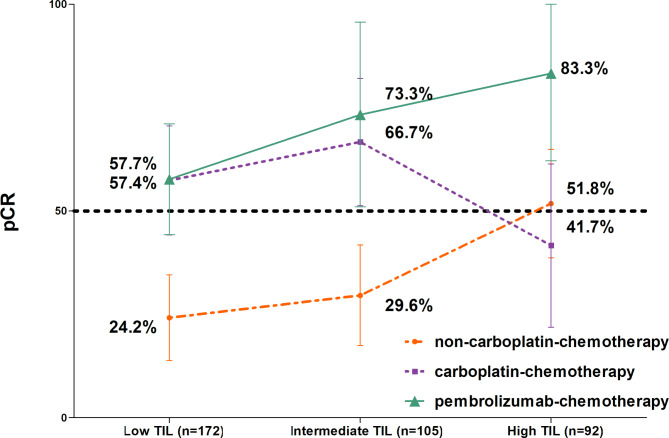
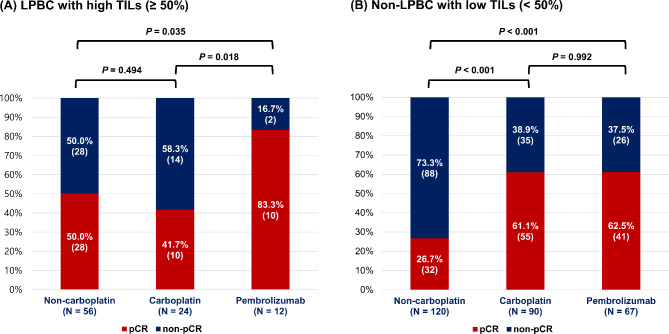
The pCR rates were 32% in the non-carboplatin-, 57% in the carboplatin-, and 64% in the pembrolizumab-chemotherapy group. Ninety-two patients (20.4%) had LPBC. In LPBC, the pCR rates did not increase with the addition of carboplatin (50.0% in the non-carboplatin and 41.7% in carboplatin) but reached 83.3% with the addition of pembrolizumab and carboplatin. Among the non-LPBC, the pCR rate increased from 26.7 to 61.1% with the addition of carboplatin, but there was no difference in the pCR rate between the carboplatin and pembrolizumab groups (61.1% and 61.2%, respectively).
In LPBC patients, the addition of carboplatin did not result in an elevated pCR rate; however, the addition of pembrolizumab tended to raise the pCR rate. In non-LPBC, the addition of carboplatin significantly increased the pCR rate, while the addition of pembrolizumab did not have the same effect.
帕博利珠单抗免疫化疗已作为高危非转移性三阴性乳腺癌(TNBC)标准治疗的一部分纳入临床实践。我们对接受新辅助化疗的TNBC患者进行了一项真实世界研究,以比较不同治疗方案(非卡铂、卡铂和帕博利珠单抗化疗)相对于基质肿瘤浸润淋巴细胞(sTIL)的病理完全缓解(pCR)率。
我们分析了2007年3月至2024年2月期间接受新辅助化疗后接受手术的450例TNBC患者队列。治疗组包括247例接受非卡铂治疗、120例接受卡铂治疗和83例接受帕博利珠单抗化疗的患者。在活检样本中评估sTIL。淋巴细胞为主型乳腺癌(LPBC)定义为sTIL高(≥50%)的肿瘤。
非卡铂治疗组的pCR率为32%,卡铂治疗组为57%,帕博利珠单抗化疗组为64%。92例患者(20.4%)患有LPBC。在LPBC中,添加卡铂后pCR率没有增加(非卡铂组为50.0%,卡铂组为41.7%),但添加帕博利珠单抗和卡铂后达到83.3%。在非LPBC中,添加卡铂后pCR率从26.7%提高到61.1%,但卡铂组和帕博利珠单抗组的pCR率没有差异(分别为61.1%和61.2%)。
在LPBC患者中,添加卡铂并未导致pCR率升高;然而,添加帕博利珠单抗倾向于提高pCR率。在非LPBC中,添加卡铂显著提高了pCR率,而添加帕博利珠单抗则没有同样的效果。