Pettenuzzo Tommaso, Ocagli Honoria, Sella Nicolò, De Cassai Alessandro, Zarantonello Francesco, Congedi Sabrina, Chiaruttini Maria Vittoria, Pistollato Elisa, Nardelli Marco, Biscaro Martina, Bassi Mara, Coniglio Giordana, Faccioli Eleonora, Rea Federico, Gregori Dario, Navalesi Paolo, Boscolo Annalisa
Institute of Anaesthesia and Intensive Care, Padua University Hospital, Padua, Italy.
Unit of Biostatistics, Epidemiology and Public Health, Department of Cardiac, Thoracic and Vascular Sciences, University of Padua, Padua, Italy.
J Anesth Analg Crit Care. 2024 Dec 18;4(1):81. doi: 10.1186/s44158-024-00214-x.
In the last decades, veno-arterial extracorporeal membrane oxygenation (V-A ECMO) has been gaining in popularity for intraoperative support during lung transplant (LT), being advocated for routinely use also in uncomplicated cases. Compared to off-pump strategy and, secondarily, to traditional cardiopulmonary bypass (CPB), V-A ECMO seems to offer a better hemodynamic stability and oxygenation, while data regarding blood product transfusions, postoperative recovery, and mortality remain unclear. This systematic review and network meta-analysis aims to evaluate the comparative efficacy and safety of V-A ECMO and CPB as compared to OffPump strategy during LT.
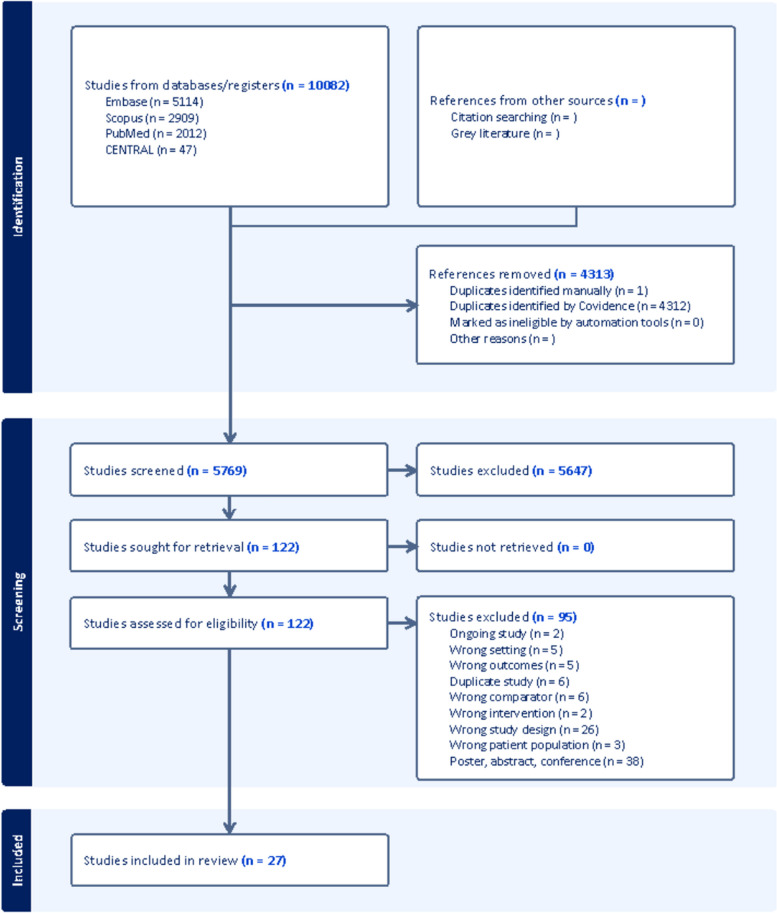
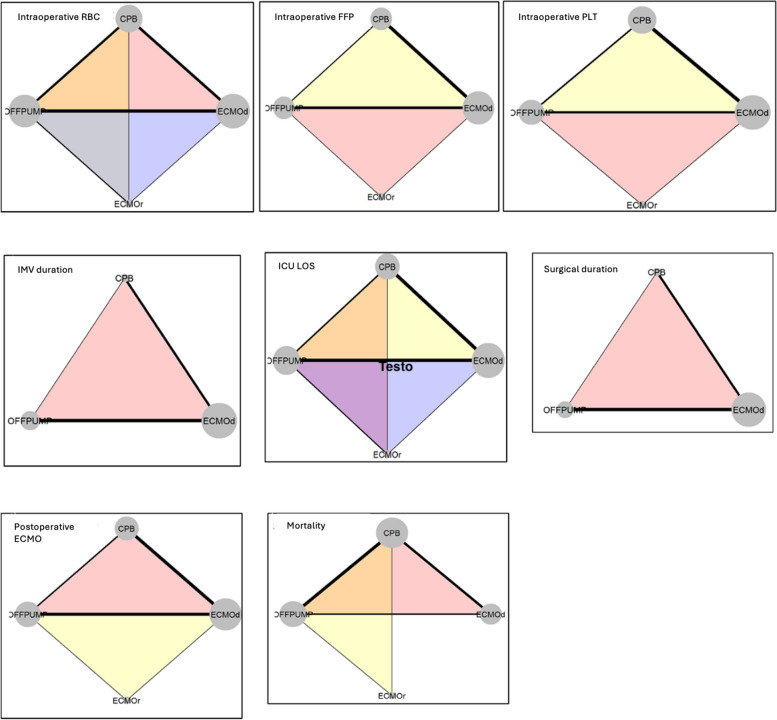
A comprehensive literature search was conducted across multiple databases (PubMed Embase, Cochrane, Scopus) and was updated in February 2024. A Bayesian network meta-analysis (NMA), with a fixed-effect approach, was performed to compare outcomes, such as intraoperative needing of blood products, invasive mechanical ventilation (IMV) duration, intensive care unit (ICU) length of stay (LOS), surgical duration, needing of postoperative ECMO, and mortality, across different supports (i.e., intraoperative V-A (default (d) or rescue (r)) ECMO, CPB, or OffPump).
Twenty-seven observational studies (6113 patients) were included. As compared to OffPump surgery, V-A ECMOd, V-A ECMOr, and CPB recorded a higher consumption of all blood products, longer IMV durations, prolonged ICU LOS, surgical duration, and higher mortalities. Comparing different extracorporeal supports, V-A ECMOd and, secondarily, V-A ECMOr overperformed CPB in nearly all above mentioned outcomes, except for RBC transfusions. The lowest rate of postoperative ECMO was recorded after OffPump surgery, while no differences were found comparing different extracorporeal supports. Finally, older age, male gender, and body mass index ≥ 25 kg/m negatively impacted on RBC transfusions, ICU LOS, surgical duration, need of postoperative ECMO, and mortality, regardless of the intraoperative extracorporeal support investigated.
This comparative network meta-analysis highlights that OffPump overperformed ECMO and CPB in all outcomes of interest, while, comparing different extracorporeal supports, V-A ECMOd and, secondarily, V-A ECMOr overperformed CPB in nearly all above mentioned outcomes, except for RBC transfusions. Older age, male gender, and higher BMI negatively affect several outcomes across different intraoperative strategies, regardless of the intraoperative extracorporeal support investigated. Future prospective studies are necessary to optimize and standardize the intraoperative management of LT.
在过去几十年中,静脉-动脉体外膜肺氧合(V-A ECMO)在肺移植(LT)术中支持方面越来越受欢迎,也被提倡在无并发症的病例中常规使用。与非体外循环策略相比,其次与传统心肺转流(CPB)相比,V-A ECMO似乎能提供更好的血流动力学稳定性和氧合,而关于血液制品输注、术后恢复和死亡率的数据仍不明确。本系统评价和网状Meta分析旨在评估LT期间V-A ECMO和CPB与非体外循环策略相比的相对疗效和安全性。
在多个数据库(PubMed、Embase、Cochrane、Scopus)中进行了全面的文献检索,并于2024年2月更新。采用固定效应方法进行贝叶斯网状Meta分析(NMA),以比较不同支持方式(即术中V-A(默认(d)或挽救(r))ECMO、CPB或非体外循环)下的术中血液制品需求、有创机械通气(IMV)持续时间、重症监护病房(ICU)住院时间(LOS)、手术持续时间、术后ECMO需求和死亡率等结果。
纳入了27项观察性研究(6113例患者)。与非体外循环手术相比,V-A ECMOd、V-A ECMOr和CPB的所有血液制品消耗量更高、IMV持续时间更长、ICU LOS延长、手术持续时间更长且死亡率更高。比较不同的体外支持方式,V-A ECMOd其次是V-A ECMOr在几乎所有上述结果方面均优于CPB,但红细胞输注除外。非体外循环手术后术后ECMO发生率最低,而比较不同的体外支持方式未发现差异。最后,无论所研究的术中体外支持方式如何,年龄较大、男性以及体重指数≥25 kg/m²对红细胞输注、ICU LOS、手术持续时间、术后ECMO需求和死亡率均有负面影响。
这项比较性网状Meta分析强调,非体外循环在所有感兴趣的结果方面均优于ECMO和CPB,而在比较不同的体外支持方式时,V-A ECMOd其次是V-A ECMOr在几乎所有上述结果方面均优于CPB,但红细胞输注除外。无论所研究的术中体外支持方式如何,年龄较大、男性以及较高的BMI对不同术中策略的多个结果均有负面影响。未来有必要进行前瞻性研究,以优化和规范LT的术中管理。