Lenz Kyle B, Watson R Scott, Wilkes Jennifer J, Keller Matthew R, Hartman Mary E, Killien Elizabeth Y
Division of Pediatric Critical Care Medicine, Department of Pediatrics, Seattle Children's Hospital, University of Washington, Seattle, WA, United States.
Center for Child Health, Behavior & Development, Seattle Children's Research Institute, Seattle, WA, United States.
Front Oncol. 2024 Dec 3;14:1501977. doi: 10.3389/fonc.2024.1501977. eCollection 2024.
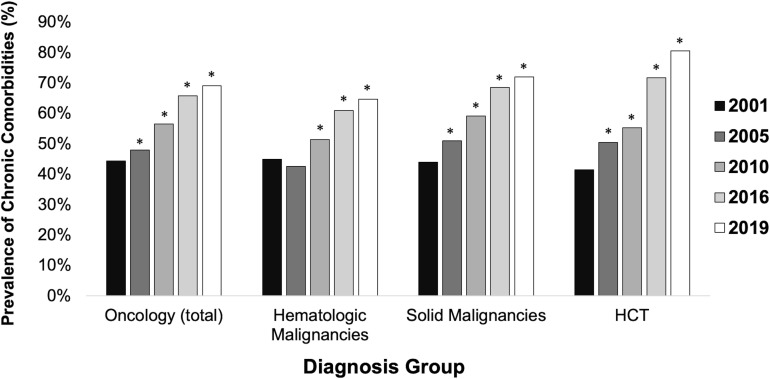
Children with cancer or hematopoietic cell transplant (HCT) frequently require ICU care. We conducted a retrospective cohort study using Healthcare Cost and Utilization Project's State Inpatient Databases from 21 U.S. states from 2001-2019. We included children <18 years with oncologic or HCT diagnosis and used ICD-9-CM and ICD-10-CM codes to identify diagnoses, comorbidities, and organ failures. We used generalized linear Poisson regression and Cuzick's test of trend to evaluate changes from 2001-2019. Among 2,157,991 total pediatric inpatient admissions, 3.9% (n=82,988) were among oncology patients and 0.3% (n=7,381) were among HCT patients. ICU admission prevalence rose from 13.6% in 2001 to 14.4% in 2019 for oncology admissions and declined from 23.9% to 19.5%, for HCT admissions. Between 2001-2019, the prevalence of chronic non-oncologic comorbidities among ICU patients rose from 44.3% to 69.1% for oncology patients (RR 1.60 [95% CI 1.46-1.66]) and from 41.4% to 81.5% (RR 1.94 [95% CI 1.61-2.34]) for HCT patients. The risk of Multiple Organ Dysfunction Syndrome more than tripled for oncology (9.5% to 33.3%; RR 3.52 [95% CI 2.97-4.18]) and HCT (12.4% to 39.7%; RR 3.20 [95% CI 2.09-4.89]) patients. Mortality decreased most for ICU patients with acute myeloid leukemia (AML) (14.6% to 8.5%) and oncology-related HCTs (15.5% to 9.2%). Critically ill pediatric oncology and HCT patients are increasingly medically complex with greater prevalence of chronic comorbidities and organ failure, but mortality did not increase. Pediatric ICUs may require increased financial and staffing support to care for these patients in the future.
患有癌症或接受造血干细胞移植(HCT)的儿童经常需要重症监护病房(ICU)护理。我们利用医疗成本和利用项目(Healthcare Cost and Utilization Project)来自美国21个州2001年至2019年的州住院数据库进行了一项回顾性队列研究。我们纳入了年龄小于18岁且诊断为肿瘤或接受造血干细胞移植的儿童,并使用国际疾病分类第九版临床修订本(ICD - 9 - CM)和国际疾病分类第十版临床修订本(ICD - 10 - CM)编码来识别诊断、合并症和器官功能衰竭。我们使用广义线性泊松回归和库齐克趋势检验来评估2001年至2019年的变化。在总共2157991例儿科住院病例中,3.9%(n = 82988)为肿瘤患者,0.3%(n = 7381)为造血干细胞移植患者。肿瘤患者的ICU入院患病率从2001年的13.6%上升至2019年的14.4%,造血干细胞移植患者的ICU入院患病率从23.9%降至19.5%。在2001年至2019年期间,ICU患者中慢性非肿瘤合并症的患病率在肿瘤患者中从44.3%升至69.1%(相对风险1.60 [95%置信区间1.46 - 1.66]),在造血干细胞移植患者中从41.4%升至81.5%(相对风险1.94 [95%置信区间1.61 - 2.34])。多器官功能障碍综合征的风险在肿瘤患者(从9.5%升至33.3%;相对风险3.52 [95%置信区间2.97 - 4.18])和造血干细胞移植患者(从12.4%升至39.7%;相对风险3.20 [95%置信区间2.09 - 4.89])中增加了两倍多。急性髓系白血病(AML)的ICU患者(从14.6%降至8.5%)和与肿瘤相关的造血干细胞移植患者(从15.5%降至9.2%)的死亡率下降最为明显。危重症儿科肿瘤和造血干细胞移植患者的医疗复杂性日益增加,慢性合并症和器官功能衰竭的患病率更高,但死亡率并未上升。未来儿科ICU可能需要增加资金和人员支持来护理这些患者。