Wen Xin, Chen Jiamin, Zhong Jing, Zhuang Yu, Deng Bixue, Lin Yuhong, Su Zhongzhen
Department of Ultrasound, the Fifth Affiliated Hospital of Sun Yat-Sen University, Zhuhai, China.
Quant Imaging Med Surg. 2024 Dec 5;14(12):8840-8851. doi: 10.21037/qims-24-1268. Epub 2024 Nov 6.
Accurate assessment of pathological complete response (pCR) to neoadjuvant chemotherapy (NAC) in breast cancer (BC) is crucial for mitigating chemotherapy-related toxicity in patients who do not respond to the treatment. Conventional ultrasound (US) has become a pivotal method for evaluating treatment response due to its cost-effectiveness, convenience, and absence of ionizing radiation. The objective of this study was to develop a model combining US and clinicopathological characteristics at baseline, as well as US features after one cycle of NAC, to predict the pCR to NAC in BC.
This retrospective study included 74 patients with invasive BC who underwent NAC from January 2022 to December 2023. Data from US and clinicopathological characteristics before NAC (pre-NAC) and US features after one cycle of NAC were collected from all patients. Univariate and multivariate analyses were used to screen the factors independently associated with pCR and to develop the prediction model. Receiver operating characteristic (ROC) curve analysis was performed, and the area under the curve (AUC), sensitivity, and specificity were calculated to assess the predictive efficiency.
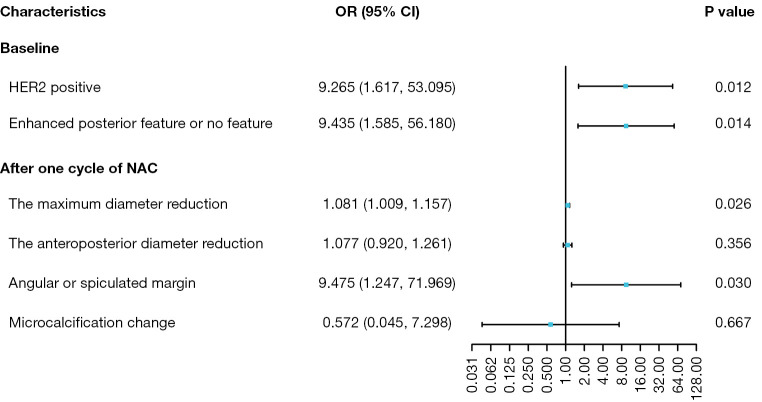
Four characteristics, including human epidermal growth factor receptor 2 (HER2)-positive [odds ratio (OR) 9.265; 95% confidence interval (CI): 1.617-53.095, P=0.012] and absence of posterior feature or posterior acoustic enhancement of the breast mass on the US pre-NAC (OR 9.435; 95% CI: 1.585-56.180, P=0.014), the maximum diameter reduction measured with the US (OR 1.081; 95% CI: 1.009-1.157, P=0.026), and the angular or spiculated margin of the breast lesion with the US after one cycle of NAC (OR 9.475; 95% CI: 1.247-71.969, P=0.030), were screened as independent predictors. The AUC, sensitivity, and specificity of the prediction model were 0.912, 90.0%, and 79.6%, respectively.
US and clinicopathological characteristics at baseline and the US features after one cycle of NAC helped predict pCR for BC. The prediction model may enable early evaluation of the efficacy of treatment strategies and guide less invasive surgical options or personalized post-treatment plans.
准确评估乳腺癌(BC)新辅助化疗(NAC)后的病理完全缓解(pCR)对于减轻对治疗无反应患者的化疗相关毒性至关重要。传统超声(US)因其成本效益、便利性和无电离辐射,已成为评估治疗反应的关键方法。本研究的目的是建立一个结合基线时的超声和临床病理特征以及NAC一个周期后的超声特征的模型,以预测BC患者对NAC的pCR。
这项回顾性研究纳入了2022年1月至2023年12月期间接受NAC的74例浸润性BC患者。收集了所有患者NAC前(NAC前)的超声和临床病理特征数据以及NAC一个周期后的超声特征。采用单因素和多因素分析筛选与pCR独立相关的因素并建立预测模型。进行了受试者操作特征(ROC)曲线分析,并计算曲线下面积(AUC)、敏感性和特异性以评估预测效率。
筛选出四个特征作为独立预测因素,包括人表皮生长因子受体2(HER2)阳性[比值比(OR)9.265;95%置信区间(CI):1.617 - 53.095,P = 0.012]、NAC前超声检查时乳腺肿块无后方特征或后方回声增强(OR 9.435;95% CI:1.585 - 56.180,P = 0.014)、超声测量的最大直径缩小(OR 1.081;95% CI:1.009 - 1.157,P = 0.026)以及NAC一个周期后超声检查时乳腺病变的边缘呈角状或毛刺状(OR 9.475;95% CI:1.247 - 71.969,P = 0.030)。预测模型的AUC、敏感性和特异性分别为0.912、90.0%和79.6%。
基线时的超声和临床病理特征以及NAC一个周期后的超声特征有助于预测BC的pCR。该预测模型可实现对治疗策略疗效的早期评估,并指导侵入性较小的手术选择或个性化的治疗后计划。