He Xu, Li Yalin, Han Dingsheng, Zhou Yanru, Zhang Jiacheng, Xu Qian, Shi Fukun, Liu Peng, Hu Hongtao, Zhang Lan
Department of Magnetic Resonance Imaging, the First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, China.
Henan University of Chinese Medicine, Zhengzhou, China.
Quant Imaging Med Surg. 2024 Dec 5;14(12):8520-8537. doi: 10.21037/qims-24-941. Epub 2024 Oct 24.
Given the limited capacity and suboptimal sensitivity of ultrasonography (US), gadoxetic acid disodium (Gd-EOB-DTPA)-enhanced magnetic resonance imaging (MRI) demonstrates good diagnostic performance for hepatocellular carcinoma (HCC). Some researchers have proposed that the abbreviated MRI (AMRI) protocols have potential as a surveillance tool. However, few studies have compared multiple AMRI protocols with complete Gd-EOB-DTPA contrast-enhanced MRI for HCC surveillance. We aimed to explore and compare the diagnostic performance of 3 AMRI protocols as HCC surveillance in high-risk patients.
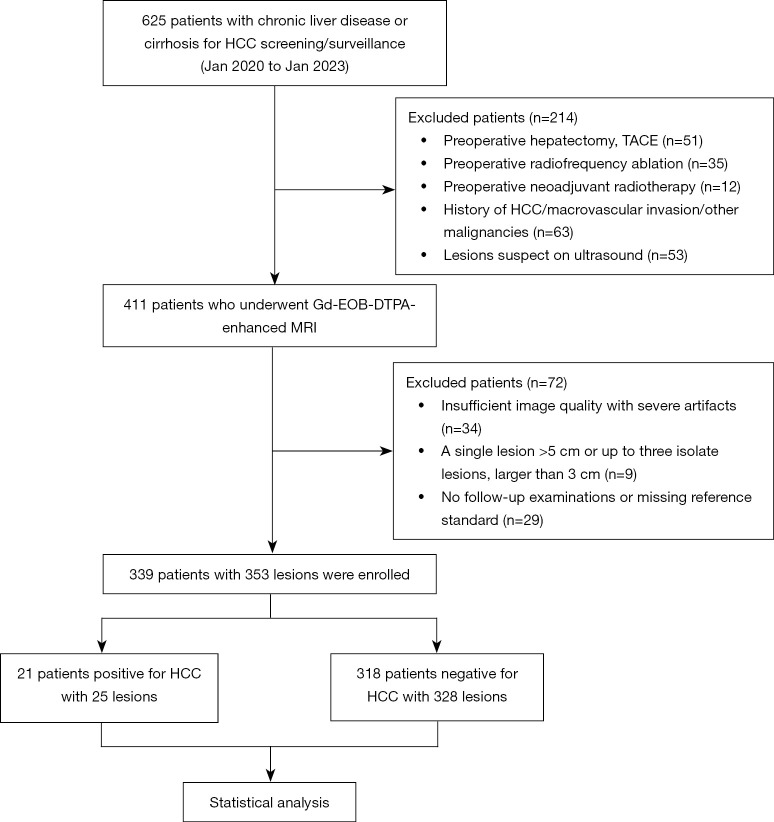
This multi-center, retrospective, blinded reader study conducted in China consecutively enrolled 339 patients with hepatitis and/or cirrhosis who underwent complete Gd-EOB-DTPA contrast-enhanced MRI for HCC surveillance from 2020 to 2023. We extracted 3 additional AMRI protocols: noncontrast-AMRI [NC-AMRI: T2-weighted imaging (T2WI) and diffusion-weighted imaging (DWI)]; dynamic-AMRI (Dyn-AMRI: early and late arterial phases, portal venous phase, and DWI); and hepatobiliary phase-AMRI (HBP-AMRI: T2WI, DWI, and HBP). Then, 2 independent radiologists assessed the AMRI and complete Gd-EOB-DTPA contrast-enhanced MRI protocols. Patients were classified as HCC positive/HCC negative based on the reference standard. Agreement was assessed using Kappa statistics. The acquisition time differences of the 4 MRI protocols were analyzed by analysis of variance (ANOVA). Per-lesion HCC diagnostic performances were compared by Cochran's Q test. Receiver operating characteristic (ROC) curves for the 3 AMRI protocols were evaluated, and the area under the ROC curve (AUROC) was calculated and compared by DeLong's test.
A total of 353 lesions were detected in the 339 included patients, and 21/339 patients were diagnosed with HCC (prevalence, 6.2%). The inter-observer agreement was good for all 4 MRI protocols (k>0.75). Acquisition times differed significantly (P<0.001), from the shortest to the longest: NC-AMRI (263.44±5.05 s) < HBP-AMRI (269.18±4.93 s) < Dyn-AMRI (307.71±4.93 s) < complete Gd-EOB-DTPA contrast-enhanced MRI (582.03±3.59 s). The sensitivity (Cochran's Q=14.667, P=0.002) and specificity (Cochran's Q=59.682, P<0.001) of 4 MRI protocols were statistically significant. HBP-AMRI showed the highest sensitivity (84.00%), whereas Dyn-AMRI exhibited the highest specificity (99.39%) among 3 AMRI protocols. The per-lesion positive predictive value (PPV) for the NC-AMRI, Dyn-AMRI, and HBP-AMRI was 41.66%, 88.89%, and 47.72%, the corresponding negative predictive value (NPV) was 96.21%, 97.31%, and 98.70%, and the number needed to diagnose (NND) for the NC-AMRI, Dyn-AMRI, HBP-AMRI, and complete Gd-EOB-DTPA contrast-enhanced MRI was: 1.865, 1.577, 1.234, and 1.569, respectively. DeLong's test showed the AUROC value of either Dyn-AMRI or HBP-AMRI was significantly higher than that of NC-AMRI (Z=2.330, P=0.019; Z=2.680, P=0.007, respectively), but no significant difference between HBP-AMRI and Dyn-AMRI (Z=1.643, P=0.100).
AMRI protocols can be implemented in clinical practice as a patient-centered and tailored regimen for HCC surveillance in China. NC-AMRI might become an optional tool due to its minimal scanning time, lower cost, and exemption from contrast agents. Dyn-AMRI, achieving the highest specificity, is a reliable surveillance strategy. HBP-AMRI as a favorable alternative showed a high sensitivity and NPV while maintaining considerable specificity and NND.
鉴于超声检查(US)的能力有限且敏感性欠佳,钆塞酸二钠(Gd-EOB-DTPA)增强磁共振成像(MRI)对肝细胞癌(HCC)具有良好的诊断性能。一些研究人员提出,简化MRI(AMRI)方案有作为监测工具的潜力。然而,很少有研究将多种AMRI方案与完整的Gd-EOB-DTPA对比增强MRI用于HCC监测进行比较。我们旨在探索和比较3种AMRI方案作为高危患者HCC监测的诊断性能。
这项在中国进行的多中心、回顾性、盲法阅片研究连续纳入了339例患有肝炎和/或肝硬化的患者,这些患者在2020年至2023年期间接受了完整的Gd-EOB-DTPA对比增强MRI以进行HCC监测。我们提取了另外3种AMRI方案:非增强AMRI [NC-AMRI:T2加权成像(T2WI)和扩散加权成像(DWI)];动态AMRI(Dyn-AMRI:动脉早期和晚期、门静脉期以及DWI);以及肝胆期AMRI(HBP-AMRI:T2WI、DWI和HBP)。然后,2名独立的放射科医生评估了AMRI和完整的Gd-EOB-DTPA对比增强MRI方案。根据参考标准将患者分类为HCC阳性/HCC阴性。使用Kappa统计量评估一致性。通过方差分析(ANOVA)分析4种MRI方案的采集时间差异。通过Cochran's Q检验比较各病变的HCC诊断性能。评估3种AMRI方案的受试者操作特征(ROC)曲线,并通过DeLong检验计算和比较ROC曲线下面积(AUROC)。
在纳入的339例患者中共检测到353个病变,21/339例患者被诊断为HCC(患病率为6.2%)。4种MRI方案的观察者间一致性均良好(k>0.75)。采集时间差异有统计学意义(P<0.001),从最短到最长依次为:NC-AMRI(263.44±5.05秒)<HBP-AMRI(269.18±4.93秒)<Dyn-AMRI(307.71±4.93秒)<完整的Gd-EOB-DTPA对比增强MRI(582.03±3.59秒)。4种MRI方案的敏感性(Cochran's Q=14.667,P=0.002)和特异性(Cochran's Q=59.682,P<0.001)有统计学意义。在3种AMRI方案中,HBP-AMRI显示出最高的敏感性(84.00%),而Dyn-AMRI表现出最高的特异性(99.39%)。NC-AMRI、Dyn-AMRI和HBP-AMRI的各病变阳性预测值(PPV)分别为41.66%、88.89%和47.72%,相应的阴性预测值(NPV)分别为96.21%、97.31%和98.70%,NC-AMRI、Dyn-AMRI、HBP-AMRI和完整的Gd-EOB-DTPA对比增强MRI的诊断所需例数(NND)分别为:1.865、1.577、1.234和1.569。DeLong检验显示,Dyn-AMRI或HBP-AMRI的AUROC值均显著高于NC-AMRI(Z=2.330,P=0.019;Z=2.680,P=0.007),但HBP-AMRI和Dyn-AMRI之间无显著差异(Z=1.643,P=0.100)。
AMRI方案可在中国作为以患者为中心的定制方案用于临床实践中的HCC监测。NC-AMRI因其扫描时间最短、成本较低且无需使用造影剂,可能成为一种可选工具。Dyn-AMRI具有最高的特异性,是一种可靠的监测策略。HBP-AMRI作为一种有利的替代方案,在保持相当特异性和NND的同时,显示出高敏感性和NPV。