From the Departments of Radiology (T.Y., G.K.), Internal Medicine (C.T.D., N.E.R., A.G.S.), and Pathology (P.G.), UT Southwestern Medical Center, 5959 Harry Hines Blvd, POB 1, Ste 420, Dallas, TX 75390-8887; Department of Biostatistics, University of Washington, Seattle, Wash (N.M.); Departments of Internal Medicine (N.D.P., T.A.J., A.S.L.) and Radiology (M.M.L., A.A., M.S.D.), University of Michigan Medical School, Ann Arbor, Mich; Departments of Diagnostic Radiology (B.F.L., C.H.L.) and Internal Medicine (K.S.), University of Maryland, Baltimore, Md; and Division of Public Health Sciences, Fred Hutch Cancer Center, Seattle, Wash (Z.F., T.L.M.).
Radiology. 2023 Apr;307(2):e220917. doi: 10.1148/radiol.220917. Epub 2023 Jan 24.
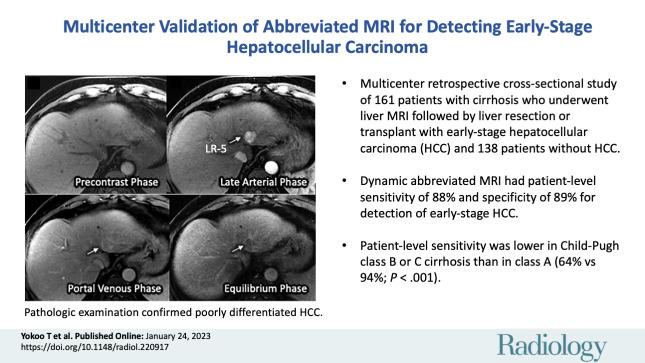
Background Abbreviated MRI is a proposed paradigm shift for hepatocellular carcinoma (HCC) surveillance, but data on its performance are lacking for histopathologically confirmed early-stage HCC. Purpose To evaluate the sensitivity and specificity of dynamic contrast-enhanced abbreviated MRI for early-stage HCC detection, using surgical pathologic findings as the reference standard. Materials and Methods This retrospective study was conducted at three U.S. liver transplant centers in patients with cirrhosis who underwent liver resection or transplant between January 2009 and December 2019 and standard "full" liver MRI with and without contrast enhancement within 3 months before surgery. Patients who had HCC-directed treatment before surgery were excluded. Dynamic abbreviated MRI examinations were simulated from the presurgical full MRI by selecting the coronal T2-weighted and axial three-dimensional fat-suppressed T1-weighted dynamic contrast-enhanced sequences at precontrast, late arterial, portal venous, and delayed phases. Two abdominal radiologists at each center independently interpreted the simulated abbreviated examinations with use of the Liver Imaging Reporting and Data System version 2018. Patients with any high-risk liver observations (>LR-3) were classified as positive; otherwise, they were classified as negative. With liver pathologic findings as the reference standard for the presence versus absence of early-stage HCC, the sensitivity, specificity, and their 95% CIs were calculated. Logistic regression was used to identify factors associated with correct classification. Results A total of 161 patients with early-stage HCC (median age, 62 years [IQR, 58-67 years]; 123 men) and 138 patients without HCC (median age, 55 years [IQR, 47-63 years]; 85 men) were confirmed with surgical pathologic findings. The sensitivity and specificity of abbreviated MRI were 88.2% (142 of 161 patients) (95% CI: 83.5, 92.5) and 89.1% (123 of 138 patients) (95% CI: 84.4, 93.8), respectively. Sensitivity was lower for Child-Pugh class B or C versus Child-Pugh class A cirrhosis (64.1% vs 94.2%; < .001). Conclusion With surgical pathologic findings as the reference standard, dynamic abbreviated MRI had high sensitivity and specificity for early-stage hepatocellular carcinoma detection in patients with compensated cirrhosis but lower sensitivity in those with decompensated cirrhosis. © RSNA, 2023 See also the editorial by Kim in this issue.
背景 对于肝细胞癌(HCC)的监测,缩短型 MRI 是一种拟议的范式转变,但在经组织病理学证实的早期 HCC 中,其性能数据仍缺乏。目的 本研究旨在评估动态对比增强缩短型 MRI 对早期 HCC 检测的灵敏度和特异性,以手术病理结果为参考标准。
材料与方法 本回顾性研究在 3 家美国肝脏移植中心进行,入组对象为 2009 年 1 月至 2019 年 12 月期间接受肝切除术或移植术且术前 3 个月内行标准“全肝”MRI 检查(包括增强和不增强)的肝硬化患者。排除术前接受 HCC 定向治疗的患者。通过选择术前全肝 MRI 的冠状位 T2 加权和轴位三维脂肪抑制 T1 加权动态对比增强序列的平扫、晚期动脉期、门静脉期和延迟期,从术前全肝 MRI 模拟缩短型 MRI 检查。每个中心的 2 位腹部放射科医生独立使用肝脏成像报告和数据系统 2018 版解读模拟缩短型 MRI 检查。将具有任何高风险肝脏观察结果(>LR-3)的患者归类为阳性;否则,将其归类为阴性。以肝脏病理结果为早期 HCC 存在与否的参考标准,计算灵敏度、特异性及其 95%置信区间。采用 logistic 回归分析确定与正确分类相关的因素。
结果 共 161 例经手术病理证实的早期 HCC 患者(中位年龄,62 岁[四分位距,58-67 岁];123 例男性)和 138 例无 HCC 患者(中位年龄,55 岁[四分位距,47-63 岁];85 例男性)的手术病理结果得到证实。缩短型 MRI 的灵敏度和特异性分别为 88.2%(161 例中的 142 例)(95%CI:83.5,92.5)和 89.1%(138 例中的 123 例)(95%CI:84.4,93.8)。Child-Pugh 分级 B 或 C 级与 A 级肝硬化相比,灵敏度较低(64.1%比 94.2%;<.001)。
结论 以手术病理结果为参考标准,动态缩短型 MRI 对代偿性肝硬化患者早期 HCC 的检测具有较高的灵敏度和特异性,但对失代偿性肝硬化患者的灵敏度较低。