Zhang Haixin, Tahami Monfared Amir Abbas, Zhang Quanwu, Honig Lawrence S
Eisai Inc., 200 Metro Blvd, Nutley, NJ, 07110, USA.
Department of Epidemiology, Biostatistics, and Occupational Health, 2001 McGill College, McGill University, Suite 1200, Montreal, QC, H3A 1G1, Canada.
Neurol Ther. 2025 Feb;14(1):319-333. doi: 10.1007/s40120-024-00695-6. Epub 2024 Dec 19.
The availability of anti-amyloid therapy for mild cognitive impairment (MCI) due to Alzheimer's disease and mild Alzheimer's dementia (AD) has underscored the need for realistic estimates of the population with AD/MCI within the healthcare system to assure adequate preparedness. We hypothesize that administrative databases can provide real-world epidemiologic estimates reflecting the population with diagnosed (known) MCI and AD. This study was conducted to estimate diagnostic incidence and prevalence of AD and all-cause MCI among the Medicare fee-for-service (FFS) and Medicare Advantage (MA) beneficiaries in the United States.
This was a retrospective analysis of Medicare beneficiaries (aged 65 and older) with identified diagnoses of AD/MCI based on ≥ 2 diagnostic codes ≥ 30 days apart. Incidence/prevalence estimates were reported per 10,000 person-years.
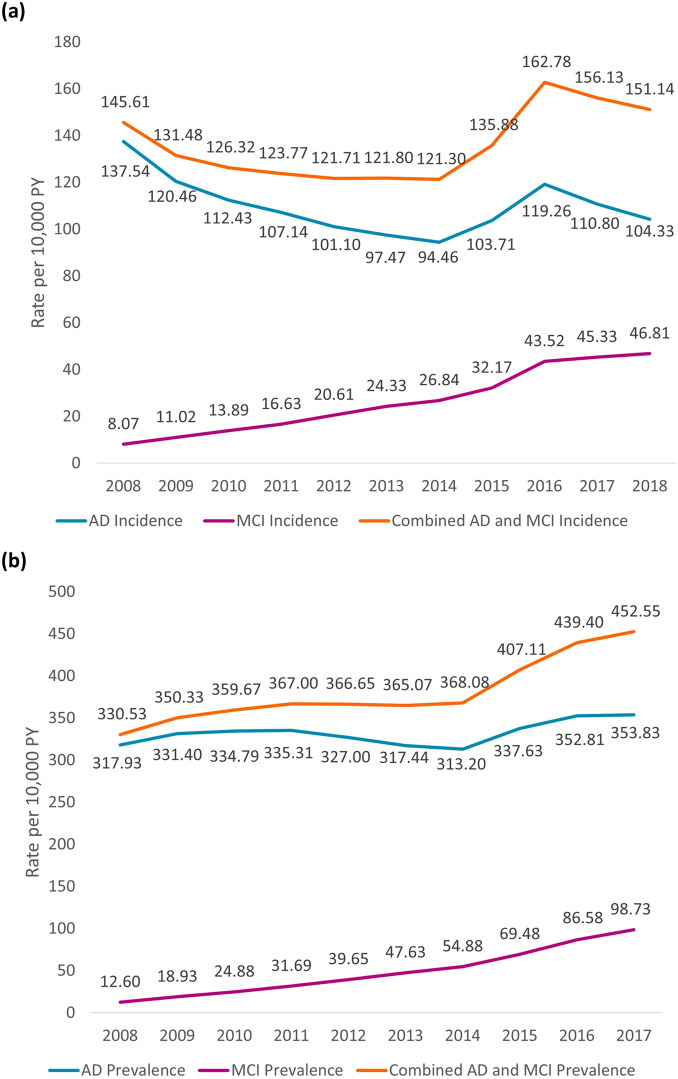
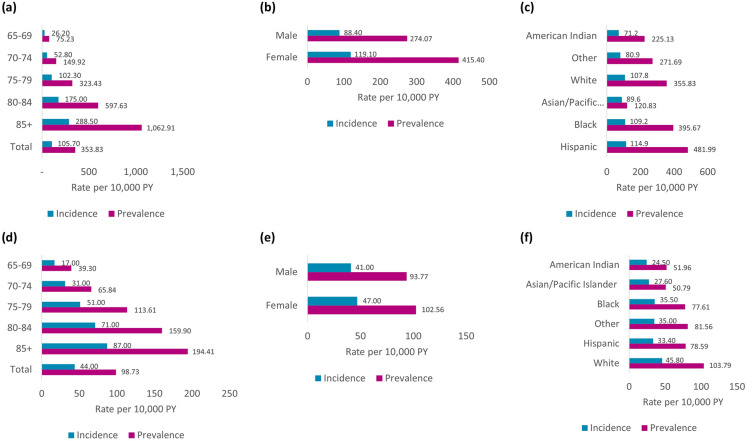
In FFS, AD incidence (2008-2018) decreased (138 to 104); MCI incidence increased (8 to 47), but the sum (MCI + AD) was relatively stable (146 to 151). Prevalence (2008-2017) increased for AD (318 to 354), and MCI (13 to 99). In MA (2016) epidemiological estimates were consistent with FFS. In 2017, older age, female sex and the Northeastern region were consistently associated with higher AD/MCI prevalence among FFS beneficiaries.
In FFS, AD/MCI diagnostic prevalence increased over 10 years, especially for MCI; prevalence estimates in MA (2016) were comparable. Diagnostic prevalence in 2016 (FFS + MA) was 3.4% for AD and 0.85% for MCI. Our findings address the reality of Alzheimer's disease in clinical practice in the United States that is confronted by healthcare professionals, payors, healthcare decision-makers, patients, and caregivers, and may offer a realistic gauge for patient triage for treatment, healthcare resource allocation, and health-systems' operational prioritization. With the availability of anti-amyloid treatments, we anticipate that the population with diagnosed MCI/AD within the Medicare database may rise over time; therefore, periodic updates of incidence/prevalence estimates may provide support for timely healthcare decision-making.
用于治疗由阿尔茨海默病引起的轻度认知障碍(MCI)和轻度阿尔茨海默病痴呆(AD)的抗淀粉样蛋白疗法的出现,凸显了在医疗保健系统中对AD/MCI患者群体进行实际估计的必要性,以确保做好充分准备。我们假设行政数据库可以提供反映已确诊(已知)MCI和AD患者群体的真实世界流行病学估计。本研究旨在估计美国医疗保险按服务收费(FFS)和医疗保险优势(MA)受益人群中AD和全因MCI的诊断发病率和患病率。
这是一项对医疗保险受益人(65岁及以上)的回顾性分析,这些受益人根据间隔≥30天的≥2个诊断代码被确定诊断为AD/MCI。发病率/患病率估计按每10,000人年报告。
在FFS中,AD发病率(2008 - 2018年)下降(从138降至104);MCI发病率上升(从8升至47),但两者之和(MCI + AD)相对稳定(从146至151)。AD患病率(2008 - 2017年)上升(从318升至354),MCI患病率也上升(从13升至99)。在MA(2016年)中,流行病学估计与FFS一致。2017年,年龄较大、女性以及东北地区在FFS受益人中一直与较高的AD/MCI患病率相关。
在FFS中,AD/MCI诊断患病率在10年期间有所上升,尤其是MCI;MA(2016年)中的患病率估计与之相当。2016年(FFS + MA)AD的诊断患病率为3.4%,MCI为0.85%。我们的研究结果反映了美国临床实践中医疗保健专业人员、付款方、医疗保健决策者、患者和护理人员所面临的阿尔茨海默病的现实情况,并可能为患者分诊治疗、医疗资源分配和卫生系统的运营优先级提供一个实际的衡量标准。随着抗淀粉样蛋白治疗方法的出现,我们预计医疗保险数据库中已确诊的MCI/AD患者群体可能会随着时间的推移而增加;因此,定期更新发病率/患病率估计可能为及时的医疗保健决策提供支持。