Choi Won Seok, Shin Jung Woo, Son Sei Wook, Kim Hak Jun, Hwang Sang Hyeon, Park Sang Geon, Park Young Hwan
Department of Orthopaedic Surgery, Korea University Guro Hospital, Seoul, South Korea.
Department of Mechatronics Convergence, Changwon National University, Changwon, South Korea.
Cartilage. 2024 Dec 20:19476035241307862. doi: 10.1177/19476035241307862.
The primary aim of this study is to examine the prevalence of ankle osteoarthritis in patients with achondroplasia and to assess the impact of surgical correction of lower limb alignment on this prevalence. The secondary aim is to identify radiographic parameters associated with ankle osteoarthritis.
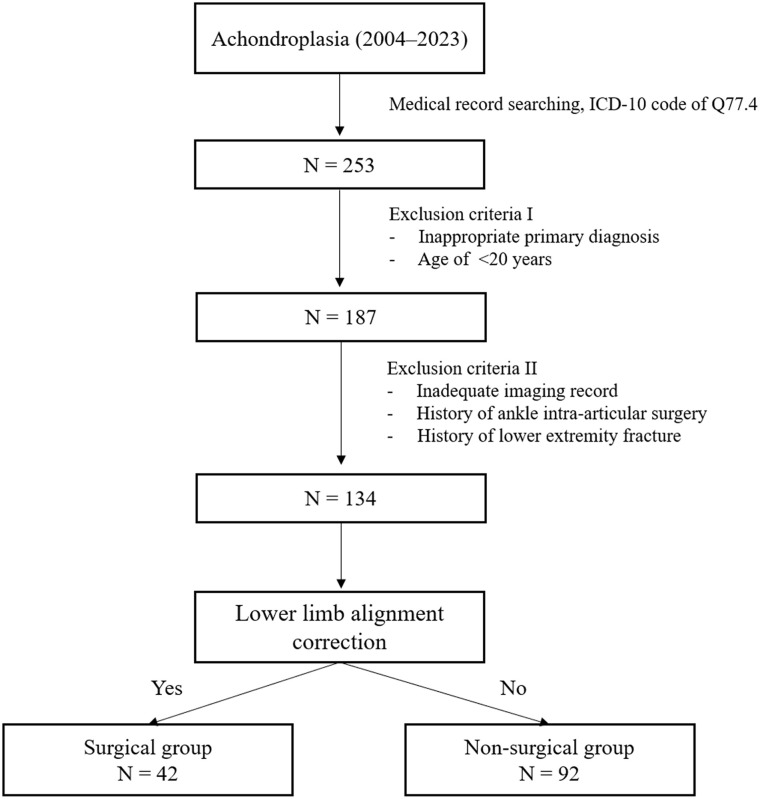
This retrospective cohort study included 134 patients (268 ankles) who visited our institution between March 2014 and February 2023. Lower limb alignment was assessed using the mechanical axis deviation, lateral distal tibial angle, anterior distal tibial angle, and talar tilt angle. Ankle osteoarthritis was evaluated using the Van Dijk Osteoarthritis score and modified Kellgren-Lawrence (K-L) scale by 2 experienced orthopedic surgeons.
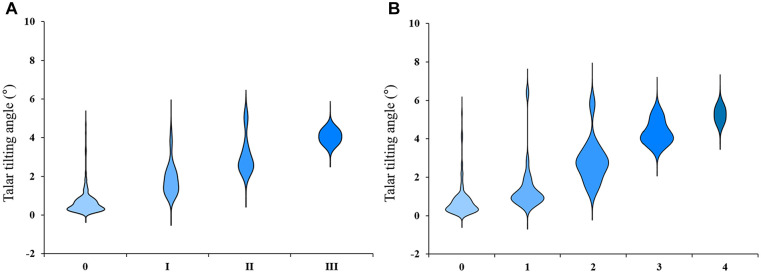
The prevalence of ankle osteoarthritis in our study cohort was 29%, and that of advanced ankle osteoarthritis defined by Van Dijk Osteoarthritis scale III or modified K-L grade 4 was 0.8% (aged <40 years, 22%, and 0%; aged ≥40 years, 42% and 2%, respectively). Talar tilt angle was the only radiographic parameter that showed a significant correlation with the degree of ankle osteoarthritis (Van Dijk Osteoarthritis score, r = 0.403, < 0.001; modified K-L grade, r = 0.385, < 0.001).
The prevalence of ankle osteoarthritis in achondroplasia is moderate, but the progression to advanced stages is uncommon. Ankle osteoarthritis in achondroplasia is strongly associated with increased talar tilt angle. This finding emphasizes caution regarding ankle osteoarthritis in achondroplasia with a nonparallel tibiotalar articular surface. Clinicians should, therefore, consider regularly assessing the talar tilt angle in patients with achondroplasia.
本研究的主要目的是调查软骨发育不全患者踝关节骨关节炎的患病率,并评估下肢力线手术矫正对此患病率的影响。次要目的是确定与踝关节骨关节炎相关的影像学参数。
这项回顾性队列研究纳入了2014年3月至2023年2月期间就诊于我院的134例患者(268个踝关节)。采用机械轴偏移、胫骨远端外侧角、胫骨远端前角和距骨倾斜角评估下肢力线。由2名经验丰富的骨科医生使用范迪克骨关节炎评分和改良的凯尔格伦-劳伦斯(K-L)分级评估踝关节骨关节炎。
在我们的研究队列中,踝关节骨关节炎的患病率为29%,根据范迪克骨关节炎量表III级或改良K-L分级4级定义的重度踝关节骨关节炎患病率为0.8%(年龄<40岁,分别为22%和0%;年龄≥40岁,分别为42%和2%)。距骨倾斜角是唯一与踝关节骨关节炎程度呈显著相关的影像学参数(范迪克骨关节炎评分,r = 0.403,<0.001;改良K-L分级,r = 0.385,<0.001)。
软骨发育不全患者踝关节骨关节炎的患病率中等,但进展至晚期并不常见。软骨发育不全患者的踝关节骨关节炎与距骨倾斜角增加密切相关。这一发现强调了对于软骨发育不全且胫距关节面不平行患者的踝关节骨关节炎需谨慎对待。因此,临床医生应考虑定期评估软骨发育不全患者的距骨倾斜角。