Kießler Maximilian, Jäger Carsten, Mota Reyes Carmen, Pergolini Ilaria, Schorn Stephan, Göß Rüdiger, Safak Okan, Martignoni Marc E, Novotny Alexander R, Uhl Waldemar, Werner Jens, Ghadimi Michael, Hartwig Werner, Ruppert Reinhard, Keck Tobias, Bruns Christiane J, Oldhafer Karl-Jürgen, Schnitzbauer Andreas, Germer Christoph-Thomas, Sommer Florian, Mees Sören Torge, Brunner Maximilian, Köninger Jörg, Glowka Tim R, Kalff Jörg C, Reißfelder Christoph, Bartsch Detlef K, Kraus Thomas, Padberg Winfried, Piso Pompiliu, Lammers Bernhard J, Rudolph Hagen, Moench Christian, Farkas Stefan, Friess Helmut, Ceyhan Güralp O, Demir Ihsan Ekin
Department of Surgery, TUM Universitätsklinikum Klinikum Rechts der Isar Technische Universität München, Ismaninger Str. 22, 81675, Munich, Germany.
German Cancer Consortium (DKTK), Partner Site, Munich, Germany.
Langenbecks Arch Surg. 2024 Dec 22;410(1):14. doi: 10.1007/s00423-024-03570-y.
Splenectomy is regularly performed in total and distal pancreatectomy due to technical reasons, lymph node dissection and radicality of the operation. However, the spleen serves as an important organ for competent immune function, and its removal is associated with an increased incidence of cancer and a worse outcome in some cancer entities (Haematologica 99:392-398, 2014; Dis Colon Rectum 51:213-217, 2008; Dis Esophagus 21:334-339, 2008). The impact of splenectomy in pancreatic cancer is not fully resolved (J Am Coll Surg 188:516-521, 1999; J Surg Oncol 119:784-793, 2019).
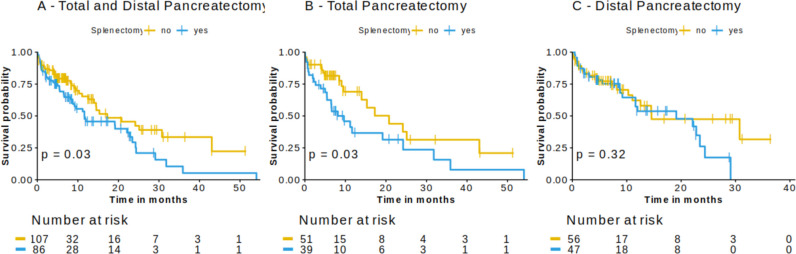
We therefore compared the outcome of 193 pancreatic cancer patients who underwent total or distal pancreatectomy with (Sp) or without splenectomy (NoSp) between 2015 and 2021 using the StuDoQ|Pancreas registry of the German Society for General and Visceral Surgery. In addition, we integrated our data into the existing literature in a meta-analysis of studies on splenectomy in pancreatic cancer patients.
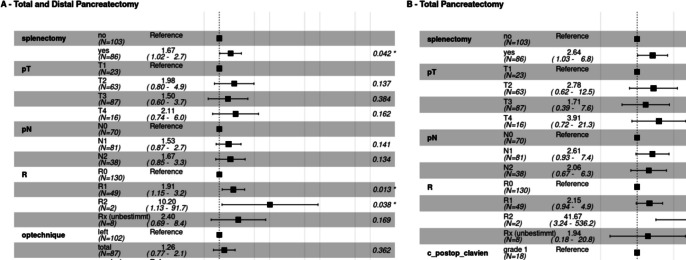
There was no difference between the Sp and NoSp groups regarding histopathological parameters, number of examined or affected lymph nodes, residual tumor status, or postoperative morbidity and mortality. We observed a significantly prolonged survival in pancreatic cancer patients who underwent total pancreatectomy, when a spleen-preserving operation was performed (median survival: 9.6 vs. 17.3 months, p = 0.03). In this group, splenectomy was identified as an independent risk factor for shorter overall survival [HR (95%CI): 2.38 (1.03 - 6.8)]. In a meta-analysis of the existing literature in combination with our data, we confirmed splenectomy as a risk factor for a shorter overall survival in pancreatic cancer patients undergoing total pancreatectomy, distal pancreatectomy, or pancreatic head resection [HR (95%CI): 1.53 (1.11 - 1.95)].
Here, we report on a strong correlations between removal of the spleen and the survival of pancreatic cancer patients undergoing total pancreatectomy. This should encourage pancreatic surgeons to critically assess the role of splenectomy in total pancreatectomy and give rise to further investigations.
由于技术原因、淋巴结清扫及手术根治性等因素,全胰切除术和胰体尾切除术常需行脾切除术。然而,脾脏是具有正常免疫功能的重要器官,切除脾脏会导致某些癌症实体的癌症发病率增加及预后变差(《血液学》99:392 - 398, 2014;《直肠肛管疾病》51:213 - 217, 2008;《食管疾病》21:334 - 339, 2008)。脾切除术对胰腺癌的影响尚未完全明确(《美国外科医师学会杂志》188:516 - 521, 1999;《外科肿瘤学杂志》119:784 - 793, 2019)。
因此,我们利用德国普通及内脏外科学会的StuDoQ|胰腺登记系统,比较了2015年至2021年间193例行全胰切除术或胰体尾切除术且有(Sp)或无脾切除术(NoSp)的胰腺癌患者的预后。此外,我们将我们的数据纳入了关于胰腺癌患者脾切除术研究的现有文献的荟萃分析中。
在组织病理学参数、检查或受累淋巴结数量、残余肿瘤状态或术后发病率和死亡率方面,Sp组和NoSp组之间没有差异。我们观察到,行保留脾脏手术的全胰切除术胰腺癌患者的生存期显著延长(中位生存期:9.6个月对17.3个月,p = 0.03)。在该组中,脾切除术被确定为总生存期较短的独立危险因素[风险比(95%置信区间):2.38(1.03 - 6.8)]。在将现有文献与我们的数据进行的荟萃分析中,我们证实脾切除术是接受全胰切除术、胰体尾切除术或胰头切除术的胰腺癌患者总生存期较短的危险因素[风险比(95%置信区间):1.53(1.11 - 1.95)]。
在此,我们报告了脾切除术与接受全胰切除术的胰腺癌患者生存期之间的强烈相关性。这应促使胰腺外科医生批判性地评估脾切除术在全胰切除术中的作用,并引发进一步的研究。