Kulkarni Ashwin J, Gunaseelan Vidhya, Brummett Chad M, Waljee Jennifer, Englesbe Michael, Bicket Mark C
From the University of Michigan Medical School, Ann Arbor, MI.
Department of Anesthesiology, University of Michigan, Ann Arbor, MI.
Ann Surg Open. 2024 Nov 7;5(4):e517. doi: 10.1097/AS9.0000000000000517. eCollection 2024 Dec.
To evaluate opioid consumption for 21 procedures over 4 years from the Michigan Surgical Quality Collaborative (MSQC) registry and update post-discharge prescribing guidelines.
Opioids remain a common treatment for postoperative pain of moderate-to-severe intensity not adequately addressed by nonopioid analgesics, but excessive prescribing correlates with increased usage. This analysis provides updates and compares patient-reported consumption in response to new guidelines.
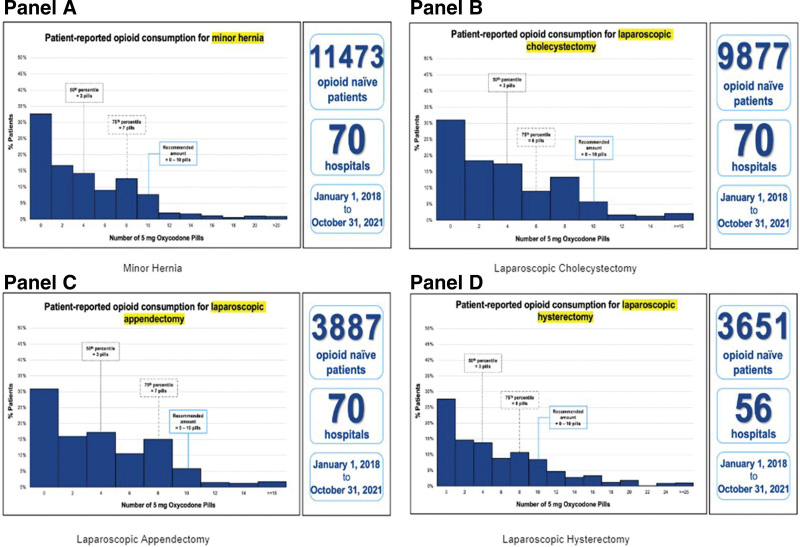
We examined data from the MSQC registry for opioid-naive adult patients undergoing surgery between January 1, 2018, and October 31, 2021. The primary outcome was patient-reported opioid consumption in oxycodone 5 mg equivalents. Guidelines were anchored to the 75th percentile of consumption, updating previous guidelines from January 2020 based on data from January 1, 2018, to May 31, 2019.
39,493 opioid-naive surgical patients (average age 53.8 years [SD 16.4], 56.3% female, 19.1% non-White, 43.9% with public insurance) were included. Guidelines did not change for 7 of the 16 procedures including the most common procedures: minor hernia, laparoscopic cholecystectomy, laparoscopic appendectomy, and laparoscopic hysterectomy. Recommended prescribing ranges were lower for 9 procedures, with most (8) procedures having a reduction of 5 pills. Prescribing guidelines were developed for 5 new procedures. All procedures had upper-limit guidelines of 10 pills or less.
For most procedures, patient-reported opioid consumption decreased between 2018 and 2021 when compared to the period between 2018 and 2019. New guidelines were established for a dozen procedures to balance maximizing pain control with reducing harms from inappropriate prescribing.
通过密歇根外科质量协作组织(MSQC)登记处评估4年中21种手术的阿片类药物使用情况,并更新出院后处方指南。
阿片类药物仍然是治疗非阿片类镇痛药无法充分缓解的中重度术后疼痛的常用方法,但过度开药与使用量增加相关。本分析提供了更新内容,并比较了患者报告的因新指南而产生的药物使用情况。
我们研究了MSQC登记处中2018年1月1日至2021年10月31日期间接受手术的未使用过阿片类药物的成年患者的数据。主要结局是患者报告的以5毫克羟考酮等效剂量计算的阿片类药物使用量。指南以使用量的第75百分位数为依据,根据2018年1月1日至2019年5月31日的数据更新了2020年1月的先前指南。
纳入了39493例未使用过阿片类药物的手术患者(平均年龄53.8岁[标准差16.4],56.3%为女性,19.1%为非白人,43.9%有公共保险)。16种手术中的7种,包括最常见的手术:小型疝气手术、腹腔镜胆囊切除术、腹腔镜阑尾切除术和腹腔镜子宫切除术,指南没有变化。9种手术的推荐处方范围降低,其中大多数(8种)手术减少了5片药。为5种新手术制定了处方指南。所有手术的上限指南均为10片或更少。
与2018年至2019年期间相比,2018年至2021年期间大多数手术患者报告的阿片类药物使用量有所下降。为十几种手术制定了新指南,以平衡最大限度地控制疼痛与减少不当开药造成的危害。