Tong Li, Li Xiaomi, Hu Mingming, Zhang Minghang, Wang Yishuo, Zhang Kai, Wang Qunhui, Zhang Tongmei, Li Baolan
Department of Oncology, Beijing Chest Hospital, Capital Medical University, Beijing, China.
Laboratory for Clinical Medicine, Capital Medical University, Beijing, China.
Ther Adv Med Oncol. 2024 Dec 19;16:17588359241307191. doi: 10.1177/17588359241307191. eCollection 2024.
Although the approval of immunotherapy in patients with extensive-stage small-cell lung cancer (ES-SCLC) has significantly improved the patient's prognosis, synchronous chemoradiotherapy has always been the standard treatment for limited-stage small-cell lung cancer (LS-SCLC).
Immuno-combined and radio-combined therapy in LS-SCLC has been applied in clinical practice, but what is the best for LS-SCLC?
This was a retrospective cohort study.
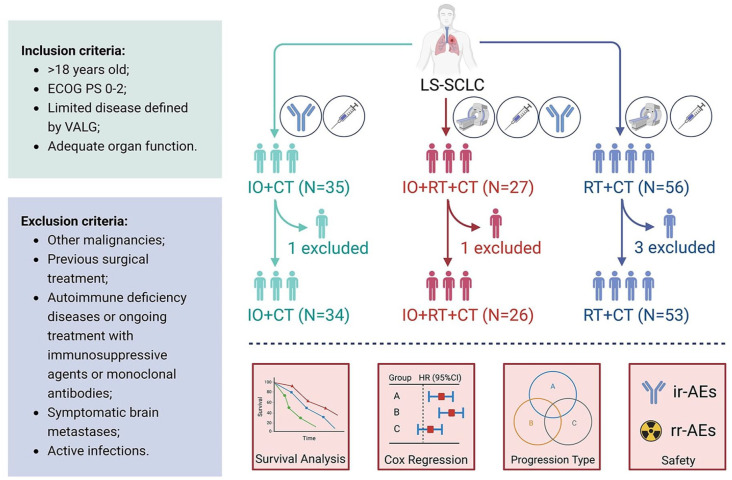
Patients with LS-SCLC from January 2019 to December 2023 were retrospectively screened and divided into three groups according to the initial treatment regimen whether included immune-combined and radio-combined treatment. Univariate and multivariate Cox regression were used to analyze the predictors affecting the survival of LS-SCLC, and the progression pattern of patients and the occurrence of adverse events (AEs) were also recorded.
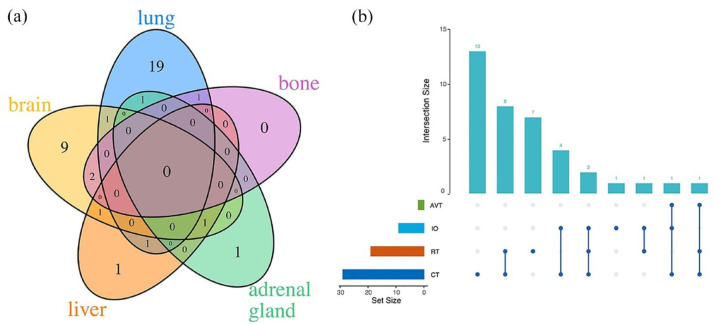
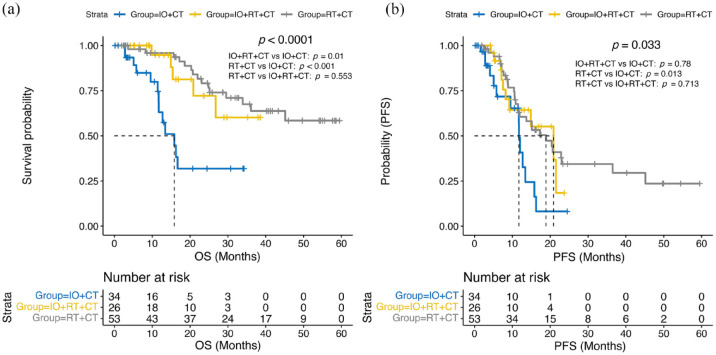
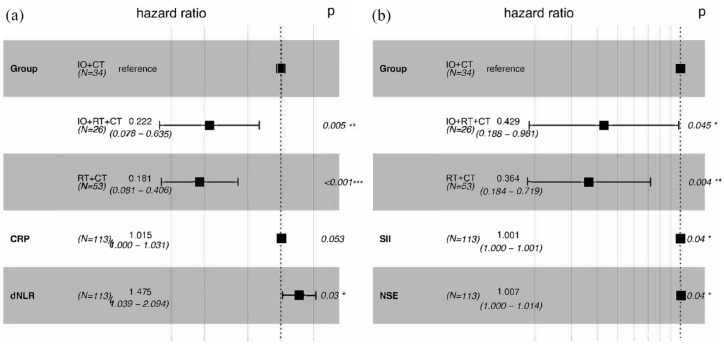
In this study, the median overall survival (OS) was 15.8 months, not yet reached (NR) and NR, and the median progression-free survival (PFS) was 11.7, 20.9, and 18.9 months in the immunotherapy combined chemotherapy ( = 34), immune combined chemoradiotherapy ( = 26), and chemoradiotherapy ( = 53) groups, respectively. OS and PFS were significantly prolonged in the radio-combined groups compared with the non-radio-combined group, and there was no significant difference between the radio-combined groups, namely immunotherapy combined chemoradiotherapy and chemoradiotherapy groups. In this study, we also constructed some indexes to predict prognosis for LS-SCLC, derived neutrophil and lymphocyte ratios were significantly associated with worse survival, and systemic inflammatory index and neuron-specific enolase (NSE) levels were significantly associated with shorter PFS. The primary organs of progression remained the lung and brain, the main immune-related AE was hypothyroidism, and the radiation-related AE was pneumonia.
Radiation-combined therapy still plays an important role in LS-SCLC in the era of immunotherapy, and clinicians cannot abandon the use of radiation therapy in the initial treatment plan for LS-SCLC.
尽管广泛期小细胞肺癌(ES-SCLC)患者免疫治疗的获批显著改善了患者预后,但同步放化疗一直是局限期小细胞肺癌(LS-SCLC)的标准治疗方法。
免疫联合和放疗联合治疗在LS-SCLC中已应用于临床实践,但哪种治疗方法对LS-SCLC最有效?
这是一项回顾性队列研究。
回顾性筛选2019年1月至2023年12月期间的LS-SCLC患者,并根据初始治疗方案是否包括免疫联合和放疗联合治疗分为三组。采用单因素和多因素Cox回归分析影响LS-SCLC生存的预测因素,并记录患者的疾病进展模式和不良事件(AE)的发生情况。
在本研究中,免疫治疗联合化疗组(n = 34)、免疫联合放化疗组(n = 26)和放化疗组(n = 53)的中位总生存期(OS)分别为15.8个月、未达到(NR)和NR,中位无进展生存期(PFS)分别为11.7、20.9和18.9个月。与非放疗联合组相比,放疗联合组的OS和PFS显著延长,放疗联合组之间无显著差异,即免疫治疗联合放化疗组和放化疗组。在本研究中,我们还构建了一些预测LS-SCLC预后的指标,衍生中性粒细胞与淋巴细胞比率与较差的生存率显著相关,全身炎症指数和神经元特异性烯醇化酶(NSE)水平与较短的PFS显著相关。进展的主要器官仍为肺和脑,主要的免疫相关AE为甲状腺功能减退,放疗相关AE为肺炎。
在免疫治疗时代,放疗联合治疗在LS-SCLC中仍发挥着重要作用,临床医生在LS-SCLC的初始治疗方案中不能放弃放疗的使用。