Ma Xiaotong, Wang Wenjuan, Yang Yumeng, Li Jiao, Wang Chenhuai, Sun Qinjian, Xia Zhangyong
Department of Neurology, Shandong Provincial Hospital, Shandong University, Jinan, Shandong, 250012, People's Republic of China.
Department of Neurology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, 250012, People's Republic of China.
J Inflamm Res. 2024 Dec 18;17:11211-11220. doi: 10.2147/JIR.S485221. eCollection 2024.
Plaque enhancement is a non-specific marker of local inflammatory response, which may offer additional insights together with circulating inflammatory markers. Few studies have analyzed the association between intracranial atherosclerotic stenosis (ICAS) plaque enhancement and circulating inflammatory markers. Given the age-related variability in the progression of ICAS, this study aims to explore the association between the two across different age groups.
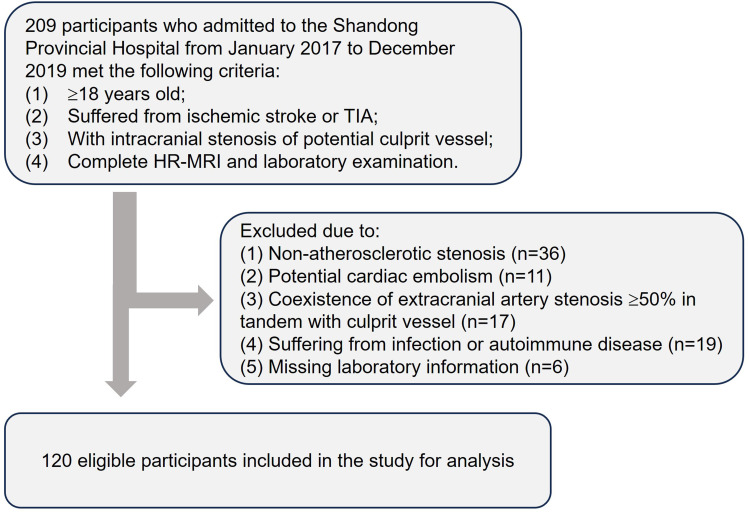
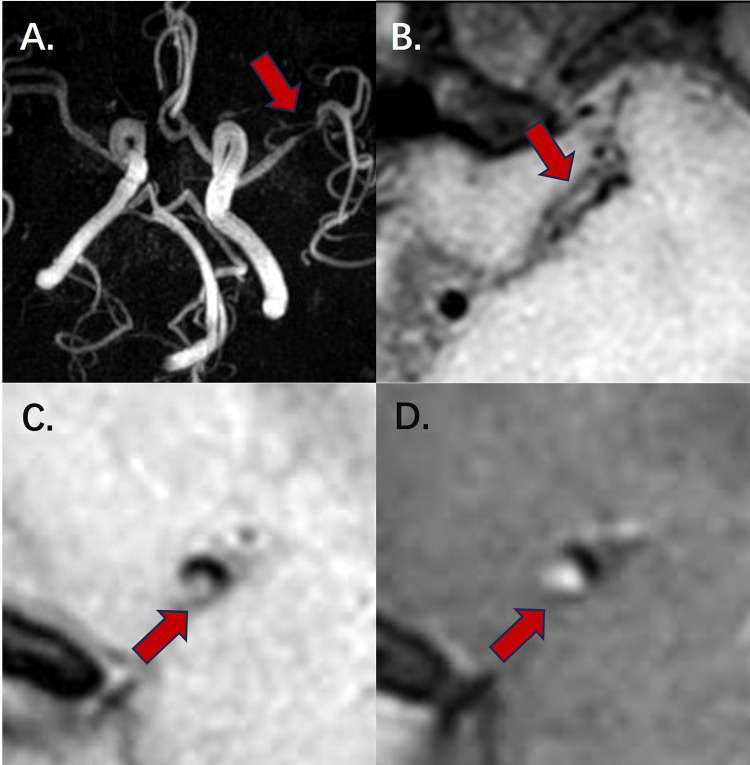
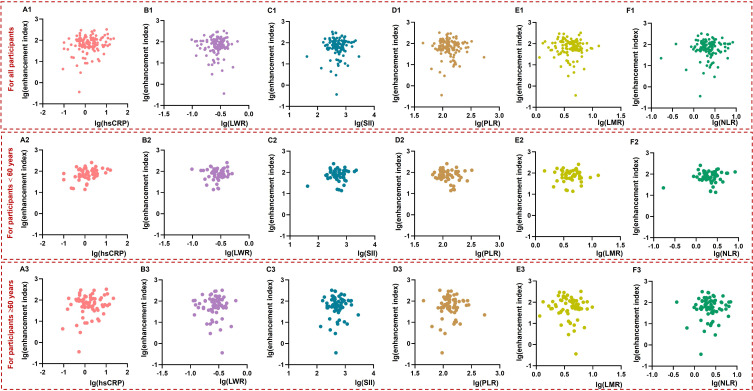
This retrospective study recruited 120 patients with ICAS-related ischemic events who had undergone high-resolution magnetic resonance imaging. Plaque enhancement index at the most stenosed site of the culprit vessel was calculated. Levels of circulating inflammatory indicators, including high-sensitivity C-reactive protein (hsCRP), lymphocyte-to-white blood cell ratio (LWR), systemic immune inflammation index (SII), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), and neutrophil-to-lymphocyte ratio (NLR), were detected. General linear regression models were established to analyze the association between ICAS plaque enhancement index and circulating inflammatory indicators.
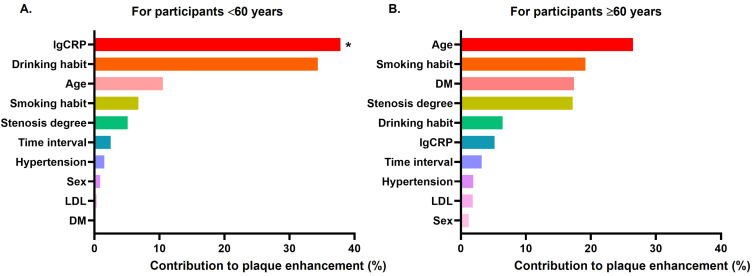
In this study, hsCRP, but not other circulating inflammatory indicators, had a significant positive association with ICAS plaque enhancement index (β=0.219, 95% CI [0.036, 0.349], =0.02). After multivariate adjustment, there was still a marginal correlation between hsCRP and the enhancement index (β=0.220, 95% CI [0.025, 0.362], =0.05). The association was particularly significant in patients <60 years rather than those ≥60 years. For participants <60 years, hsCRP had the highest contribution to plaque enhancement interpretation.
ICAS plaque enhancement index was positively associated with hsCRP, particularly in participants aged <60 years. This may be helpful for understanding the significance of the enhancement index in clinical practice.
斑块强化是局部炎症反应的非特异性标志物,它可能与循环炎症标志物一起提供更多信息。很少有研究分析颅内动脉粥样硬化狭窄(ICAS)斑块强化与循环炎症标志物之间的关联。鉴于ICAS进展存在年龄相关的变异性,本研究旨在探讨不同年龄组中两者之间的关联。
这项回顾性研究纳入了120例因ICAS相关缺血事件而接受高分辨率磁共振成像的患者。计算罪犯血管最狭窄部位的斑块强化指数。检测循环炎症指标水平,包括高敏C反应蛋白(hsCRP)、淋巴细胞与白细胞比值(LWR)、全身免疫炎症指数(SII)、血小板与淋巴细胞比值(PLR)、淋巴细胞与单核细胞比值(LMR)以及中性粒细胞与淋巴细胞比值(NLR)。建立一般线性回归模型以分析ICAS斑块强化指数与循环炎症指标之间的关联。
在本研究中,hsCRP与ICAS斑块强化指数呈显著正相关,而其他循环炎症指标则无此关联(β = 0.219,95%可信区间[0.036, 0.349],P = 0.02)。多因素调整后,hsCRP与强化指数之间仍存在边缘相关性(β = 0.220,95%可信区间[0.025, 0.362],P = 0.05)。这种关联在年龄<60岁的患者中尤为显著,而非≥60岁的患者。对于年龄<60岁的参与者,hsCRP对斑块强化解释的贡献最大。
ICAS斑块强化指数与hsCRP呈正相关,尤其是在年龄<60岁的参与者中。这可能有助于在临床实践中理解强化指数的意义。