Takahashi Makoto, Sakamoto Kazuhiro, Ro Hisashi, Kochi Saki, Toake Miyuki, Takahashi Hiromitsu, Irie Takahiro, Momose Hirotaka, Amemiya Kota, Tsuchiya Yuki, Tsukamoto Ryoichi, Honjo Kumpei, Kawai Masaya, Ishiyama Shun, Sugimoto Kiichi, Kojima Yutaka
Department of Coloproctological Surgery, Juntendo University Faculty of Medicine, Tokyo, Japan.
BMC Surg. 2024 Dec 23;24(1):416. doi: 10.1186/s12893-024-02697-5.
Lateral lymph node dissection (LLND) for locally advanced rectal cancer (LARC) is performed widely since it reduces local recurrence. However, there are some disadvantages to LLND, including technical difficulties and association with postoperative urinary dysfunction. Procedures for LARC have also become more minimally invasive: laparoscopic surgery (LS) has become more common, and use of robot-assisted LS (RALS) is increasing. The purpose of this study is to assess differences in postoperative urinary dysfunction after LLND for LARC between LS and RALS, and to identify risk factors for postoperative urinary dysfunction.
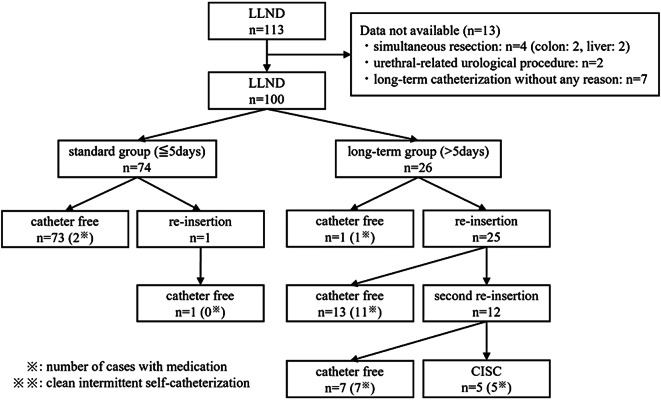
The subjects were 100 patients with LARC (≥ cT3) with the inferior border of the tumor reaching the peritoneal reflection who underwent LS or RALS with LLND between 2009 and 2023 at Juntendo University Hospital. After LLND, the urinary catheter was usually removed on or before postoperative day 5. The duration of urinary catheterization (DUC) was used to evaluate postoperative urinary dysfunction. The standard (S) and long-term (L) groups were defined as cases with urinary catheter removal at ≤ 5 and > 5 days, respectively. DUC was examined for LS vs. RALS and clinicopathological factors were identified that adversely affect DUC.
Of the 100 subjects, 72 underwent LS and 28 received RALS. LLND was bilateral in 65 cases and unilateral in 35 cases. The median DUC was 5 days, with 74 cases in group S and 26 in group L. The most frequent postoperative complication (Clavien-Dindo Grade 2 or higher) was urinary dysfunction, followed by ileus and surgical site infection (SSI), and none differed by procedure (LS vs. RALS). Univariate analysis showed significant differences in LLND laterality (p = 0.02) and SSI (p = 0.04) between groups S and L. In multivariate analysis, bilateral LLND (p < 0.01, HR 7.37) and SSI (p = 0.01, HR 15.36) were independent factors that worsened DUC.
There was no difference in urinary dysfunction after LLND between LS and RALS. Bilateral LLND and SSI were risk factors for lengthening DUC. Compared to bilateral LLND, unilateral LLND can reduce urinary dysfunction; therefore, selective LLND, which is overwhelmingly unilateral LLND, and prevention of perioperative SSI may be important for maintenance of urinary function.
局部晚期直肠癌(LARC)的侧方淋巴结清扫术(LLND)因能降低局部复发率而被广泛应用。然而,LLND存在一些缺点,包括技术难度大以及与术后排尿功能障碍相关。LARC的手术方式也变得更加微创:腹腔镜手术(LS)已更为常见,机器人辅助腹腔镜手术(RALS)的应用也在增加。本研究的目的是评估LARC患者在接受LLND后,LS与RALS术后排尿功能障碍的差异,并确定术后排尿功能障碍的危险因素。
研究对象为100例LARC(≥cT3)患者,肿瘤下缘达腹膜反折,于2009年至2023年在顺天堂大学医院接受了LLND的LS或RALS手术。LLND术后,导尿管通常在术后第5天或之前拔除。导尿管留置时间(DUC)用于评估术后排尿功能障碍。标准(S)组和长期(L)组分别定义为导尿管在≤5天和>5天拔除的病例。比较LS与RALS的DUC情况,并确定对DUC有不利影响的临床病理因素。
100例研究对象中,72例接受了LS,28例接受了RALS。LLND双侧65例,单侧35例。DUC中位数为5天,S组74例,L组26例。最常见的术后并发症(Clavien-Dindo 2级或更高)是排尿功能障碍,其次是肠梗阻和手术部位感染(SSI),不同手术方式(LS与RALS)之间无差异。单因素分析显示,S组和L组在LLND侧别(p = 0.02)和SSI(p = 0.04)方面存在显著差异。多因素分析显示,双侧LLND(p < 0.01,HR 7.37)和SSI(p = 0.01,HR 15.36)是使DUC恶化的独立因素。
LS与RALS在LLND术后的排尿功能障碍方面无差异。双侧LLND和SSI是延长DUC的危险因素。与双侧LLND相比,单侧LLND可减少排尿功能障碍;因此,绝大多数为单侧LLND的选择性LLND以及围手术期SSI的预防对于维持排尿功能可能很重要。