Huang Qiming, Chen Shai, Xiao Yuanyuan, Chen Wei, He Shancheng, Xie Baochang, Zhao Wenqi, Xu Yuhui, Luo Guiping
Department of Cardiac Surgery, The Second Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang, Jiangxi, China.
Department of Vascular Surgery, The Second Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang, Jiangxi, China.
Front Surg. 2024 Dec 9;11:1506850. doi: 10.3389/fsurg.2024.1506850. eCollection 2024.
Lung cancer is the leading cause of cancer-related mortality. Lymph node involvement remains a crucial prognostic factor in non-small cell lung cancer (NSCLC), and the TNM system is the current standard for staging. However, it mainly considers the anatomical location of lymph nodes, neglecting the significance of node count. Metrics like metastatic lymph node count and lymph node ratio (LNR) have been proposed as more accurate predictors.
We used data from the SEER 17 Registry Database (2010-2019), including 52,790 NSCLC patients who underwent lobectomy or pneumonectomy, with at least one lymph node examined. Primary outcomes were overall survival (OS) and cancer-specific survival (CSS). Cox regression models assessed the prognostic value of negative lymph node (NLN) count, number of positive lymph node (NPLN), and LNR, with cut-points determined using X-tile software. Model performance was evaluated by the Akaike information criterion (AIC).
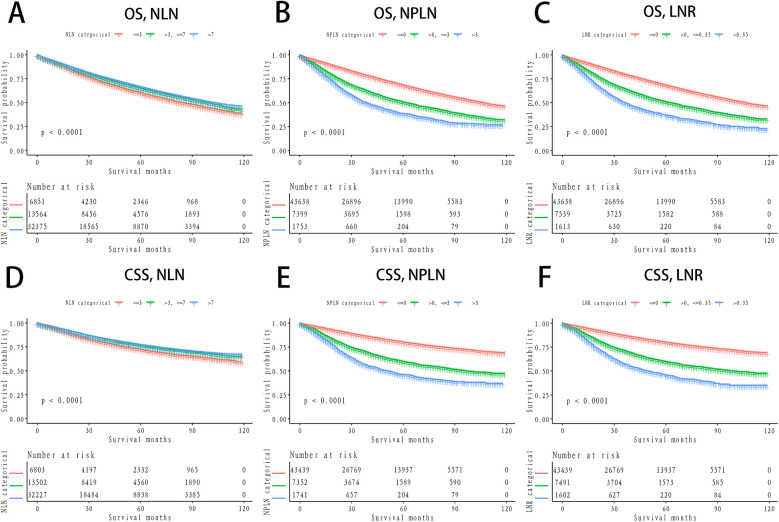
The Cox proportional hazards model analysis revealed that NLN, NPLN, and LNR are independent prognostic factors for OS and LCSS ( < 0.0001). Higher NLN counts were associated with better survival (HR = 0.79, 95% CI = 0.76-0.83, < 0.0001), while higher NPLN (HR = 2.19, 95% CI = 1.79-2.67, < 0.0001) and LNR (HR = 1.64, 95% CI = 1.79-2.67, < 0.0001) values indicated worse outcomes. Kaplan-Meier curves for all three groups (NLN, NPLN, LNR) demonstrated clear stratification ( < 0.0001). The NLN-based model (60,066.5502) exhibited the strongest predictive performance, followed by the NPLN (60,508.8957) and LNR models (60,349.4583), although the differences in AIC were minimal.
NLN count, NPLN, and LNR were all identified as independent prognostic indicators in patients with NSCLC. Among these, the predictive model based on NLN demonstrated a marginally superior prognostic value compared to NPLN, with NPLN outperforming the LNR model. Notably, higher NLN counts, along with lower NPLN and LNR values, were consistently associated with improved survival outcomes. The relationship between these prognostic markers and NSCLC survival warrants further validation through prospective studies.
肺癌是癌症相关死亡的主要原因。淋巴结受累仍然是非小细胞肺癌(NSCLC)的关键预后因素,而TNM系统是目前的分期标准。然而,它主要考虑淋巴结的解剖位置,而忽略了淋巴结数量的意义。已提出转移淋巴结计数和淋巴结比率(LNR)等指标作为更准确的预测指标。
我们使用了SEER 17注册数据库(2010 - 2019年)的数据,包括52790例行肺叶切除术或全肺切除术且至少检查了一个淋巴结的NSCLC患者。主要结局为总生存期(OS)和癌症特异性生存期(CSS)。Cox回归模型评估阴性淋巴结(NLN)计数、阳性淋巴结数量(NPLN)和LNR的预后价值,使用X-tile软件确定切点。通过赤池信息准则(AIC)评估模型性能。
Cox比例风险模型分析显示,NLN、NPLN和LNR是OS和LCSS的独立预后因素(<0.0001)。较高的NLN计数与更好的生存期相关(HR = 0.79,95%CI = 0.76 - 0.83,<0.0001),而较高的NPLN(HR = 2.19,95%CI = 1.79 - 2.67,<0.0001)和LNR(HR = 1.64,95%CI = 1.79 - 2.67,<0.0001)值表明预后较差。所有三组(NLN、NPLN、LNR)的Kaplan-Meier曲线显示出明显的分层(<0.0001)。基于NLN的模型(60066.5502)表现出最强的预测性能,其次是NPLN(60508.8957)和LNR模型(60349.4583),尽管AIC的差异很小。
NLN计数、NPLN和LNR均被确定为NSCLC患者的独立预后指标。其中,基于NLN的预测模型与NPLN相比显示出略优的预后价值,NPLN优于LNR模型。值得注意的是,较高的NLN计数以及较低的NPLN和LNR值始终与改善的生存结局相关。这些预后标志物与NSCLC生存之间的关系值得通过前瞻性研究进一步验证。