Wang Yaxin, Wang Qingyun, Ren Hanyun, Dong Yujun, Wang Qingya, Liang Zeyin, Yin Yue, Liu Wei, Xu Weilin, Han Na, Li Yuan
Department of Hematology, Peking University First Hospital, Beijing, China.
Front Oncol. 2024 Dec 9;14:1465334. doi: 10.3389/fonc.2024.1465334. eCollection 2024.
Acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS) constitute myeloid malignancies, and allogeneic hematopoietic stem cell transplantation (allo-HSCT) is considered as a potentially optimal approach for achieving a long term cure. However, post-allo-HSCT relapse remains a leading cause of mortality and therapeutic failure.
To evaluate the efficacy and safety of combining hypomethylating agents (HMAs) with Bcl-2 inhibitors in the treatment of AML/MDS relapse following allo-HSCT, we retrospectively collected data from 42 patients who experienced relapse between April 2012 and March 2022 at Peking University First Hospital. Among these patients, 21 underwent intensive chemotherapy (IC) alone, while the other 21 received treatment with HMAs after IC treatment, either alone or in combination with the Bcl-2 inhibitor venetoclax (VEN).
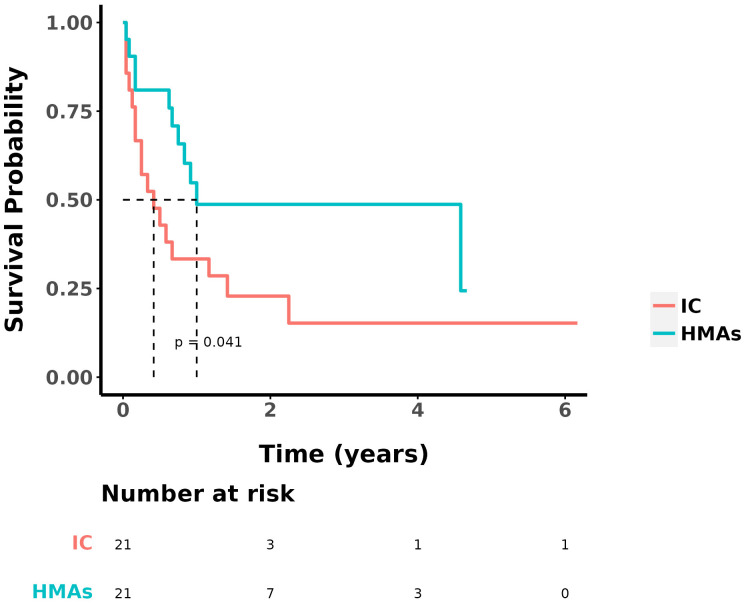
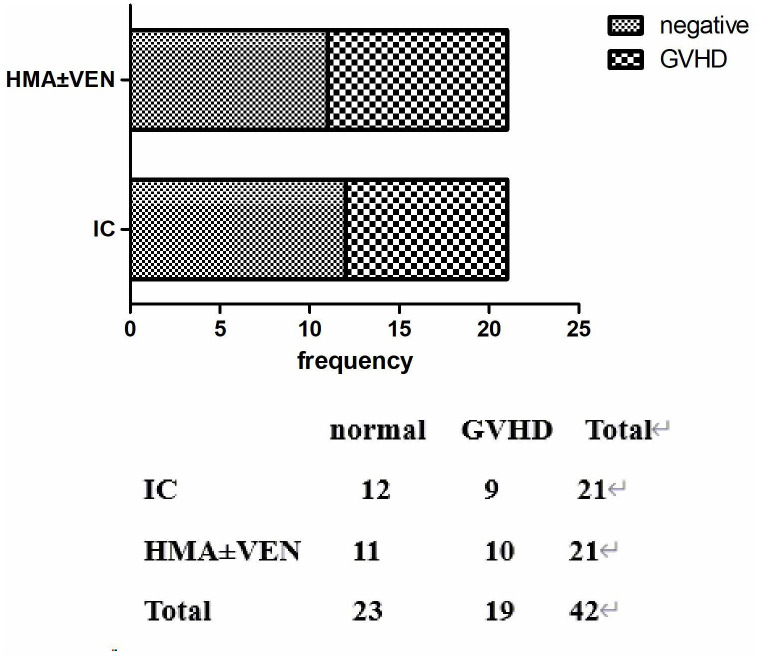
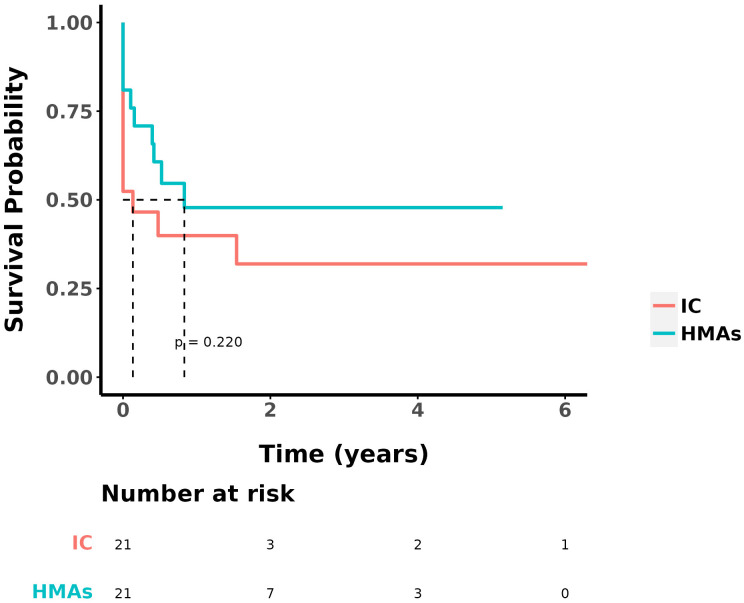
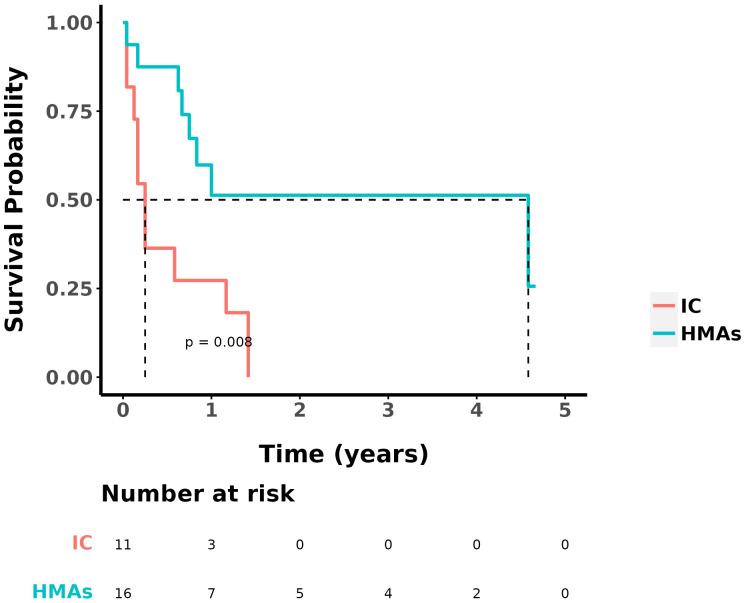
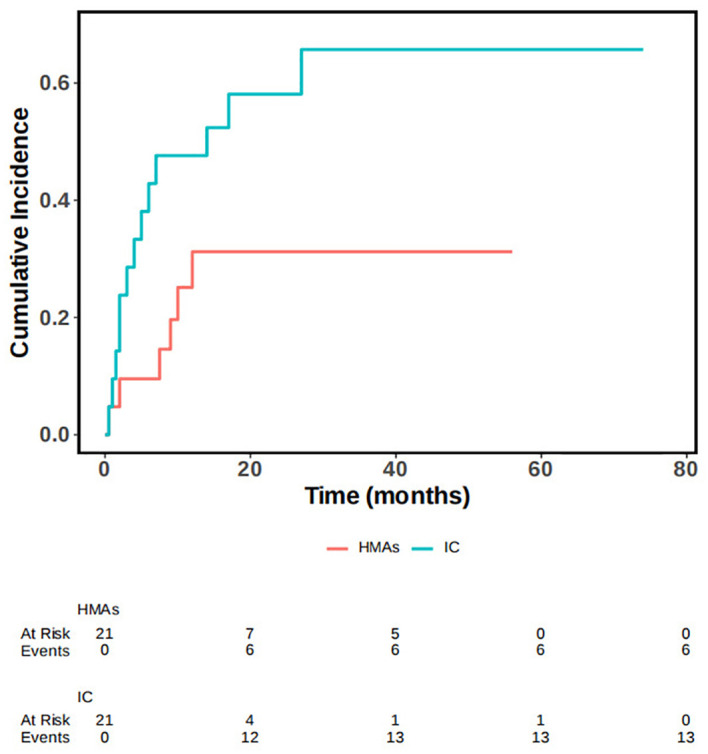
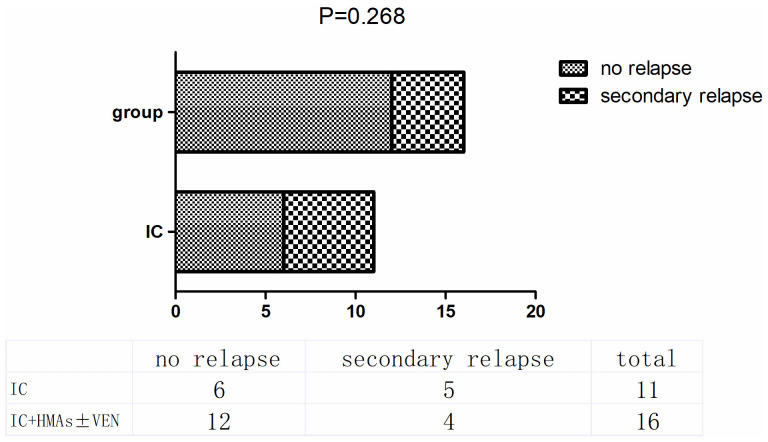
The median overall survival (OS) was 9 ± 2.153 months, and the one-year OS rate was 41.5%. The overall response rate (ORR) in the chemotherapy group and the IC+HMAs ± VEN group was 52.38% (11/21) and 76.19% (16/21), respectively, with no significant difference found (P=0.107). Kaplan-Meier analysis revealed a significant difference in OS between the chemotherapy group and the IC+HMAs ± VEN group in our retrospective cohort study (P=0.041, χ2= 4.016). Additionally, a significant difference in overall survival (OS) rates was observed between the two groups for patients categorized as intermediate/high risk (P=0.008). The secondary relapse rate was 45.45% (5/11) in the IC cohort and 25% (4/16) in the IC+HMAs ± VEN group, respectively, with no significant difference identified between the two cohorts (P=0.268). Furthermore, upon assessing the risk of graft-versus-host disease (GvHD), infection, and agranulocytosis, no notable differences were observed with the use of HMAs, suggesting that HMAs did not increase the risk. In the IC+HMAs ± VEN group, 7 patients received VEN in addition to HMAs, and no significant statistical difference was found in OS when comparing patients who received HMAs alone and those who received HMA+VEN (P=0.183), also, a statistically significant difference in OS was noted between the two groups whenaccounting for competing risks (P=0.028).
This retrospective study highlights the efficacy of IC+HMAs ± VEN in treating AML/MDS patients experiencing relapse post allo-HSCT, improving survival rates, especially for those classified as intermediate/high risk, with favorable tolerability.
急性髓系白血病(AML)和骨髓增生异常综合征(MDS)构成髓系恶性肿瘤,异基因造血干细胞移植(allo-HSCT)被认为是实现长期治愈的潜在最佳方法。然而,allo-HSCT后复发仍然是死亡和治疗失败的主要原因。
为了评估去甲基化药物(HMAs)与Bcl-2抑制剂联合治疗allo-HSCT后AML/MDS复发的疗效和安全性,我们回顾性收集了2012年4月至2022年3月期间在北京大学第一医院复发的42例患者的数据。在这些患者中,21例仅接受强化化疗(IC),另外21例在IC治疗后接受HMAs治疗,单独使用或与Bcl-2抑制剂维奈克拉(VEN)联合使用。
中位总生存期(OS)为9±2.153个月,一年OS率为41.5%。化疗组和IC+HMAs±VEN组的总缓解率(ORR)分别为52.38%(11/21)和76.19%(16/21),未发现显著差异(P=0.107)。Kaplan-Meier分析显示,在我们的回顾性队列研究中,化疗组和IC+HMAs±VEN组之间的OS存在显著差异(P=0.041,χ2=4.016)。此外,在分类为中/高风险的患者中,两组之间的总生存率(OS)也观察到显著差异(P=0.008)。IC队列中的二次复发率为45.45%(5/11),IC+HMAs±VEN组为25%(4/16),两组之间未发现显著差异(P=0.268)。此外,在评估移植物抗宿主病(GvHD)、感染和粒细胞缺乏症的风险时,使用HMAs未观察到明显差异,这表明HMAs不会增加风险。在IC+HMAs±VEN组中,7例患者除接受HMAs外还接受了VEN,比较单独接受HMAs的患者和接受HMA+VEN的患者时,OS未发现显著统计学差异(P=0.183),此外,在考虑竞争风险时,两组之间的OS也存在统计学显著差异(P=0.028)。
这项回顾性研究强调了IC+HMAs±VEN在治疗allo-HSCT后复发的AML/MDS患者中的疗效,提高了生存率,特别是对于那些分类为中/高风险的患者,且耐受性良好。