McEvoy Alannah, Rodrigues Myanca, Dennis Brittany B, Hudson Jacqueline, Marsh David C, Worster Andrew, Thabane Lehana, Samaan Zainab
Department of Psychiatry and Behavioural Neurosciences, McMaster University, 100 West 5th St., Hamilton, ON L8N 3K7, Canada.
Department of Health Research Methods, Evidence, and Impact, McMaster University, 1280 Main St. W, Hamilton, ON L8S 4L8, Canada.
Addict Behav Rep. 2024 Nov 27;21:100575. doi: 10.1016/j.abrep.2024.100575. eCollection 2025 Jun.
The substance use crisis continues to progress. Medication for Opioid Use Disorder (MOUD) are prescribed to reduce opioid use and related harms; however, many individuals continue to use substances while on treatment. The objective of this study was to describe the temporal and demographic trends of the agreement between self-reported and urine tested substances.
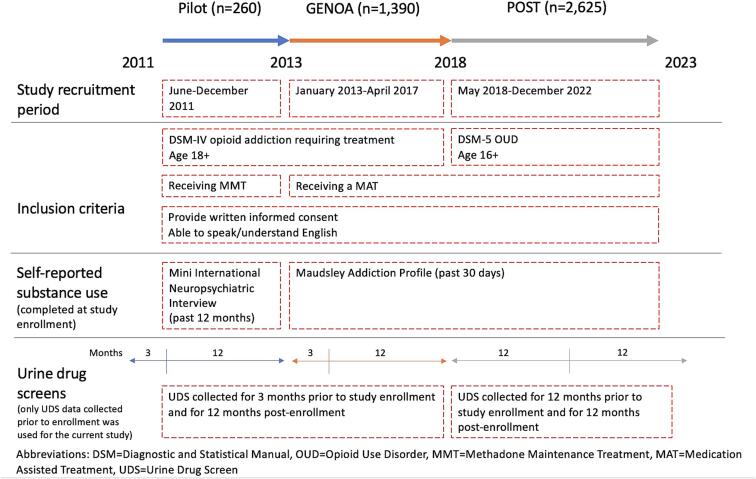
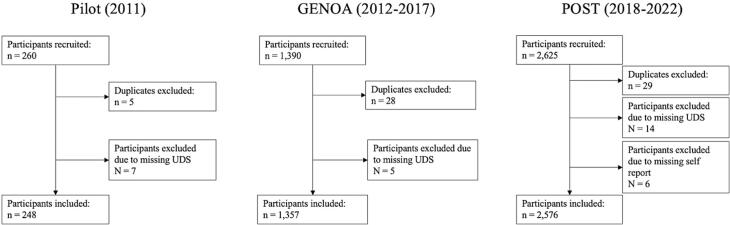
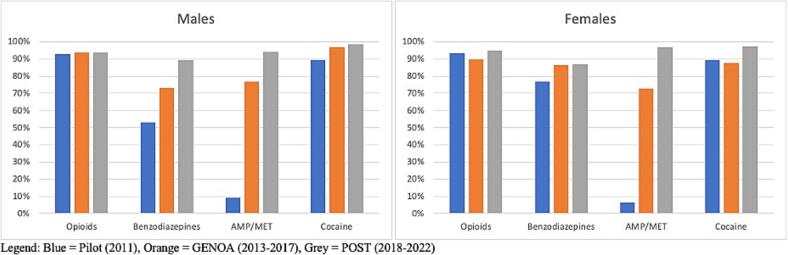
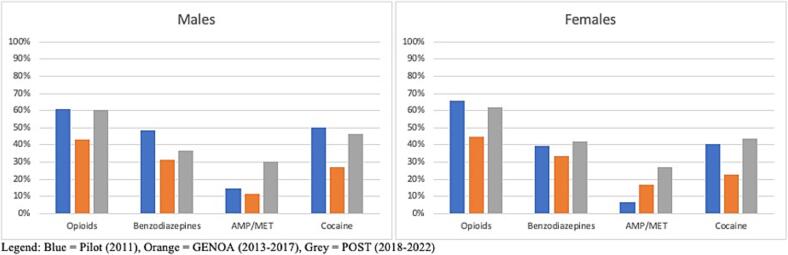
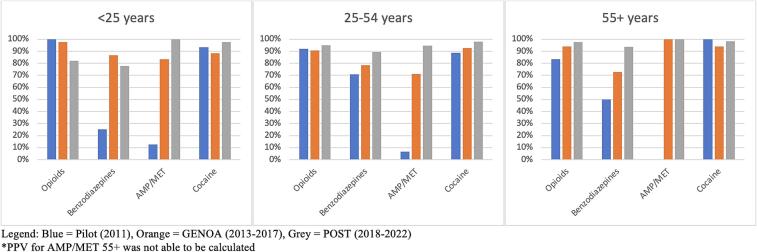
The current study is a retrospective secondary analysis of three phases of a prospective cohort study (Pilot 2011, Genetics of opioid addiction (GENOA) 2013-2017, and Pharmacogenetics of opioid substitution treatment (POST)) 2018-2022) spanning 2011-2022. We compared the self-reported substance use data for opioids, benzodiazepines, amphetamine/methamphetamine (AMP/MET), and cocaine with urine drug results. We compared the positive predictive value (PPV), false omission rate (FOR), sensitivity, and specificity between (i) different drugs; (ii) by sex, and (iii) age group at enrollment in each phase of the study using self-reported substance use at baseline and retrospective electronic health record data on urine drug screenings collected over the same time period.
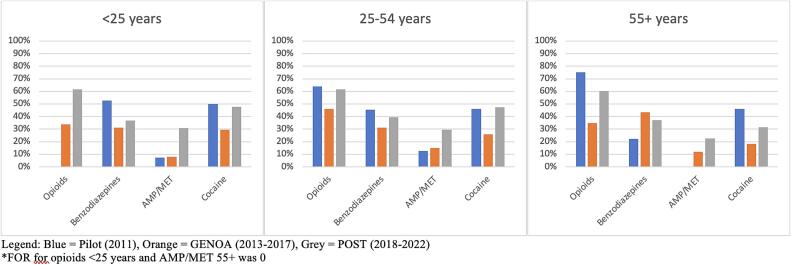
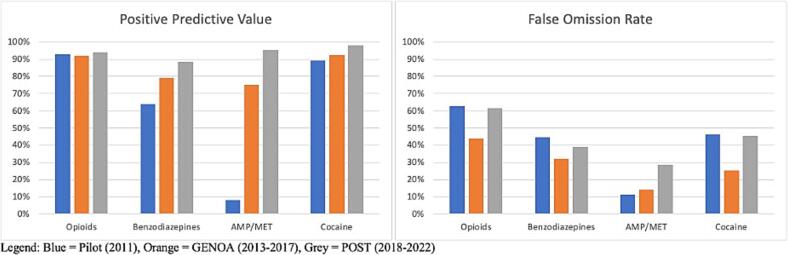
Overall, the average PPV and FOR for any drug across all phases was 80.7 % and 37.9 %, respectively. Sensitivity and specificity were highest for cocaine and lowest for benzodiazepines. We found no specific trend by sex. Lastly, we found a higher sensitivity for opioids and AMP/MET in those under 25 years of age compared to other age groups. PPV increased over time for benzodiazepines, AMP/MET and cocaine and FOR was higher during the pilot and POST phases than the GENOA phase.
Our study highlights the unique challenges associated with ascertaining substance use behaviour for individuals receiving MOUD, indicating many patients will accurately report substance use while others do not. It is therefore important to consider the context of the patient, and the type of the co-substance used to select patient-centred testing as indicated. Therefore, the answer to the question of do we need urine drug screen is yes in some cases.
物质使用危机仍在持续发展。阿片类物质使用障碍药物(MOUD)被用于减少阿片类物质使用及相关危害;然而,许多个体在接受治疗期间仍继续使用物质。本研究的目的是描述自我报告的物质使用情况与尿液检测结果之间一致性的时间和人口统计学趋势。
本研究是对一项前瞻性队列研究三个阶段(2011年试点阶段、2013 - 2017年阿片类成瘾遗传学(GENOA)阶段以及2018 - 2022年阿片类替代治疗药物遗传学(POST)阶段)的回顾性二次分析,研究跨度为2011 - 2022年。我们将阿片类物质、苯二氮䓬类药物、苯丙胺/甲基苯丙胺(AMP/MET)和可卡因的自我报告物质使用数据与尿液药物检测结果进行了比较。我们使用基线时的自我报告物质使用情况以及同期收集的尿液药物筛查回顾性电子健康记录数据,比较了(i)不同药物之间;(ii)按性别;(iii)各研究阶段入组时年龄组之间的阳性预测值(PPV)、漏诊率(FOR)、敏感性和特异性。
总体而言,所有阶段中任何药物的平均PPV和FOR分别为80.7%和37.9%。可卡因的敏感性和特异性最高,苯二氮䓬类药物最低。我们未发现按性别划分的特定趋势。最后,我们发现与其他年龄组相比,25岁以下人群对阿片类物质和AMP/MET的敏感性更高。苯二氮䓬类药物、AMP/MET和可卡因的PPV随时间增加,且试点阶段和POST阶段的FOR高于GENOA阶段。
我们的研究突出了确定接受MOUD治疗个体物质使用行为所面临的独特挑战,表明许多患者会准确报告物质使用情况,而其他患者则不会。因此,重要的是要考虑患者的背景以及所使用的共物质类型,以便按指示选择以患者为中心的检测方法。所以,在某些情况下,我们是否需要进行尿液药物筛查这个问题的答案是肯定的。