Jin Yue, Yang Fei, Rank Christopher M, Letovsky Stanley, Ramge Peter, Jochum Simon
Roche Information Solutions, Roche Molecular Systems Inc, 2881 Scott Blvd, Santa Clara, CA, 95050, USA.
Roche Information Solutions, F. Hoffman-La Roche Ltd, Basel, Switzerland.
Infect Dis Ther. 2025 Jan;14(1):229-243. doi: 10.1007/s40121-024-01090-2. Epub 2024 Dec 26.
The use of antibody titers against SARS-CoV-2, as a method of estimating subsequent infection following infection or vaccination, is unclear. Here, we investigate whether specific levels of antibodies, as markers of adaptive immunity, can serve to estimate the risk of symptomatic SARS-CoV-2 (re-) infection.
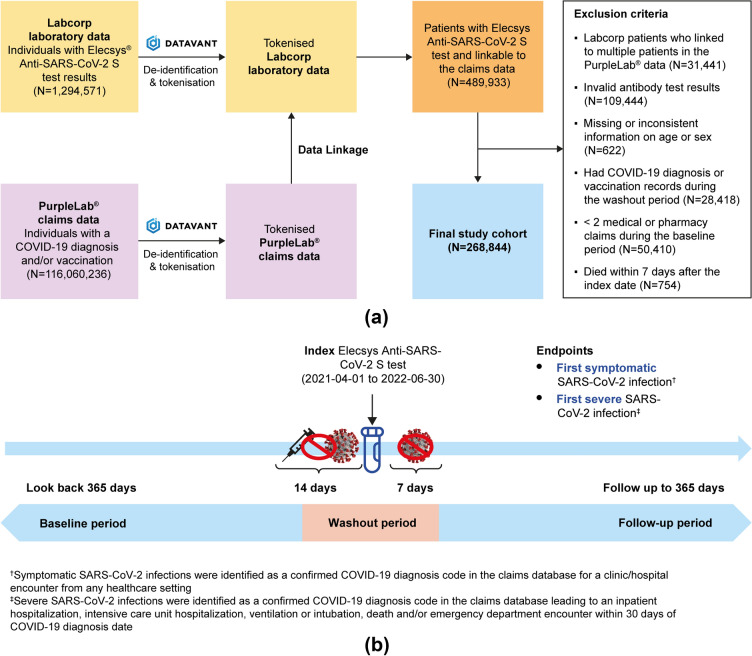
In this real-world study, laboratory data from individuals tested for SARS-CoV-2 antibodies under routine clinical conditions were linked through tokenization to a United States medical insurance claims database to determine the risk of symptomatic/severe SARS-CoV-2 infection outcomes. Antibody titer levels were determined using the Elecsys Anti-SARS-CoV-2 S assay. Study outcomes included the first symptomatic SARS-CoV-2 infection (per ICD-10 diagnostic codes, occurring ≥ 7 days post-antibody titer test), and severe SARS-CoV-2 infection, characterized by adverse outcomes including hospitalization, intensive care unit admission, intubation, mechanical ventilation, or death within 30 days of infection. All outcomes were assessed for 12 months following antibody measurement. Hazard ratios of subsequent symptomatic and severe infections were estimated using Cox regression with inverse probability weighting.
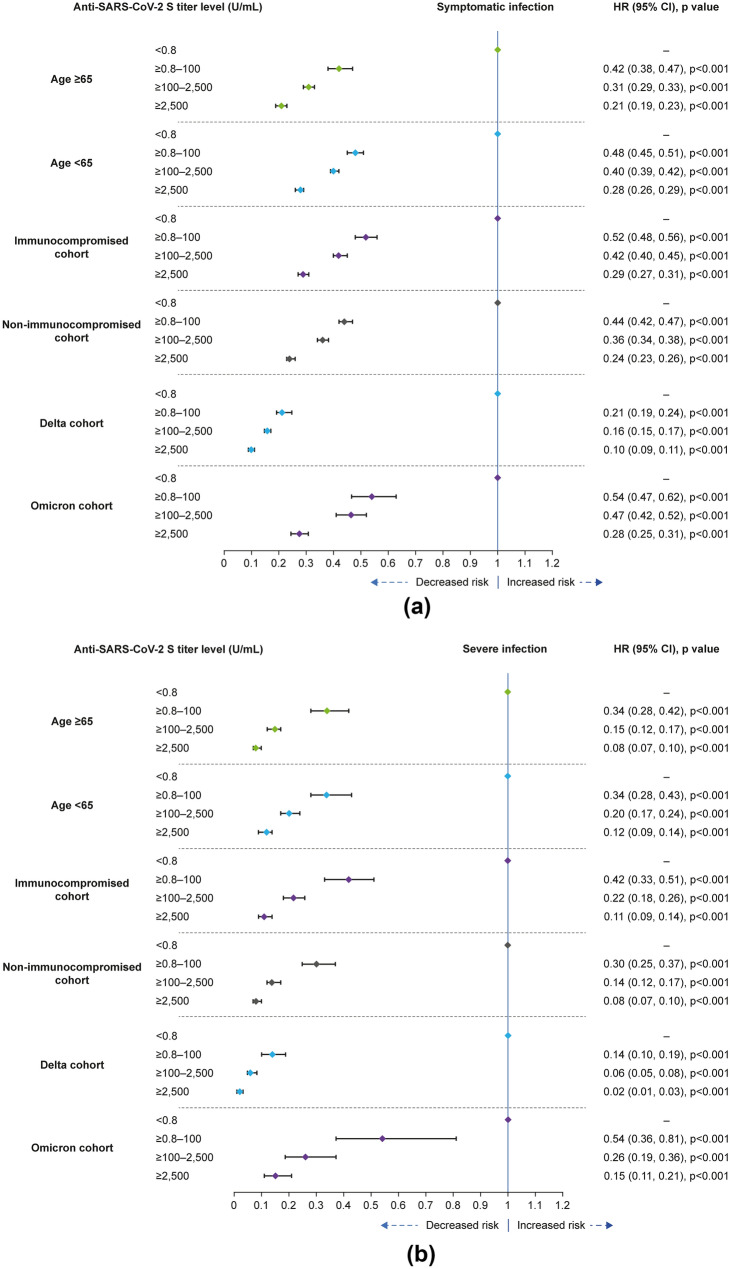
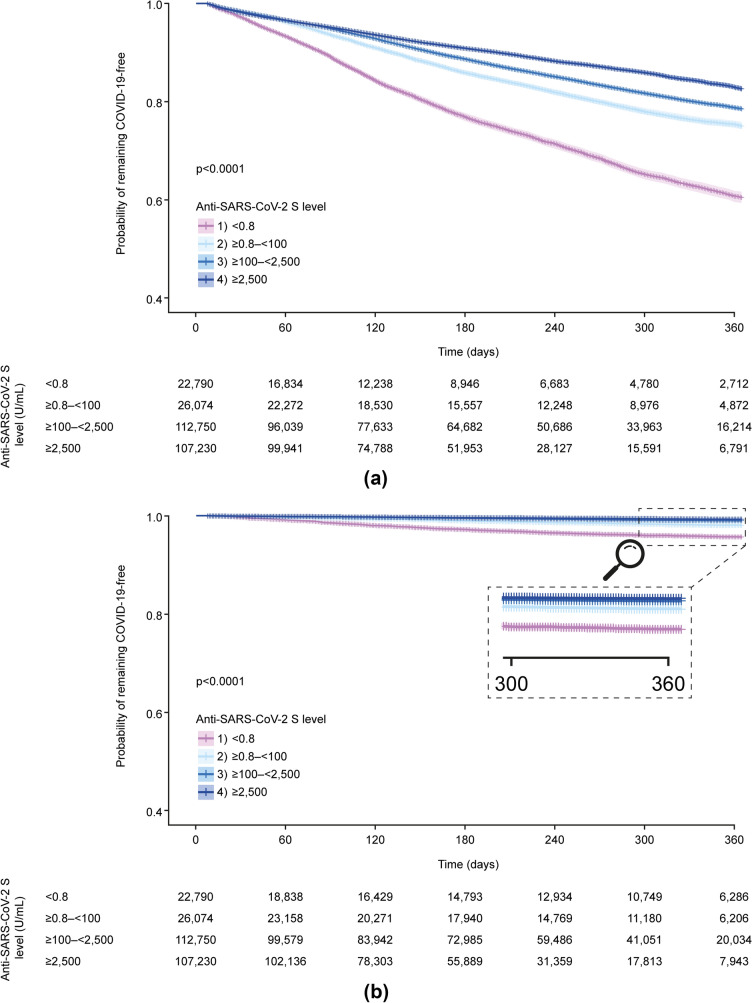
Of 268,844 individuals with antibody data (April 2021-June 2022), those with levels ≥ 0.8 to < 1,000 U/mL had a 42% reduced risk of symptomatic infection within 12 months, compared with < 0.8 U/mL (HR = 0.58, 95% CI [0.55, 0.61]). The risk decreased by 53% (HR = 0.47, 95% CI [0.45, 0.49]) with ≥ 1000 to < 2500 U/mL and by 62% (HR = 0.38 [0.36, 0.39]) for ≥ 2500 U/mL. Risk of severe SARS-CoV-2 outcomes was also reduced. Subgroup analyses showed a consistent association between antibody levels and infection risk, by immune status and age. Clinically meaningful thresholds of antibody titers varied between Delta and Omicron infections.
Higher antibody titer levels indicated reduced risk of developing symptomatic or severe COVID-19. Titers of ≥ 2500 U/mL indicated a 62-87% reduced infection risk. The quantitative determination of antibody titers allowed scaling of the correlate of risk to new variants.
使用针对严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的抗体滴度作为估计感染或接种疫苗后后续感染的方法尚不清楚。在此,我们研究作为适应性免疫标志物的特定抗体水平是否可用于估计有症状的SARS-CoV-2(再)感染风险。
在这项真实世界研究中,在常规临床条件下接受SARS-CoV-2抗体检测的个体的实验室数据通过令牌化与美国医疗保险理赔数据库相关联,以确定有症状/严重SARS-CoV-2感染结局的风险。使用Elecsys抗SARS-CoV-2 S检测法测定抗体滴度水平。研究结局包括首次有症状的SARS-CoV-2感染(根据国际疾病分类第十版诊断编码,在抗体滴度检测后≥7天发生)以及严重SARS-CoV-2感染,其特征为感染后30天内出现包括住院、重症监护病房收治、插管、机械通气或死亡等不良结局。在抗体检测后的12个月内评估所有结局。使用带逆概率加权的Cox回归估计后续有症状和严重感染的风险比。
在268,844名有抗体数据的个体(2021年4月至2022年6月)中,抗体水平≥0.8至<1000 U/mL的个体在12个月内出现有症状感染的风险比抗体水平<0.8 U/mL的个体降低了42%(风险比=0.58,95%置信区间[0.55, 0.61])。抗体水平≥1000至<2500 U/mL时风险降低了53%(风险比=0.47,95%置信区间[0.45, 0.49]),≥2500 U/mL时风险降低了62%(风险比=0.38[0.36, 0.39])。严重SARS-CoV-2感染结局的风险也降低了。亚组分析显示,按免疫状态和年龄分层,抗体水平与感染风险之间存在一致的关联。抗体滴度的临床有意义阈值在德尔塔毒株和奥密克戎毒株感染之间有所不同。
较高的抗体滴度水平表明发生有症状或严重新型冠状病毒肺炎(COVID-19)的风险降低。滴度≥2500 U/mL表明感染风险降低了62%至87%。抗体滴度的定量测定使得能够将风险关联指标应用于新的病毒变体。