Chung Jaeyeon, Koo Chang-Hoon, Park Jungchan, Kim Hye-Bin, Bae Jinyoung, Ju Jae-Woo, Lee Soowon, Oh Ah Ran, Kim Hyo Sung, Park Soo Jung, Jeon Yunseok, Nam Karam
Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, Seoul National University College of Medicine, 101 Daehak-Ro, Jongno-Gu, Seoul, 03080, Republic of Korea.
Department of Anesthesiology and Pain Medicine, Seoul National University Bundang Hospital, Seongnam, Gyeonggi Province, Republic of Korea.
Trials. 2024 Dec 26;25(1):850. doi: 10.1186/s13063-024-08707-4.
Intraoperative hypotension is very common during surgery and is linked to major organ dysfunction and mortality. Current perioperative blood pressure management is largely based on universal blood pressure thresholds ranging from a mean arterial pressure of 60-70 mmHg. However, the effectiveness of this conventional management remains unproven in prospective randomized trials. Therefore, we will conduct this study to test if individualized perioperative blood pressure management decreases the incidence of postoperative major adverse outcomes.
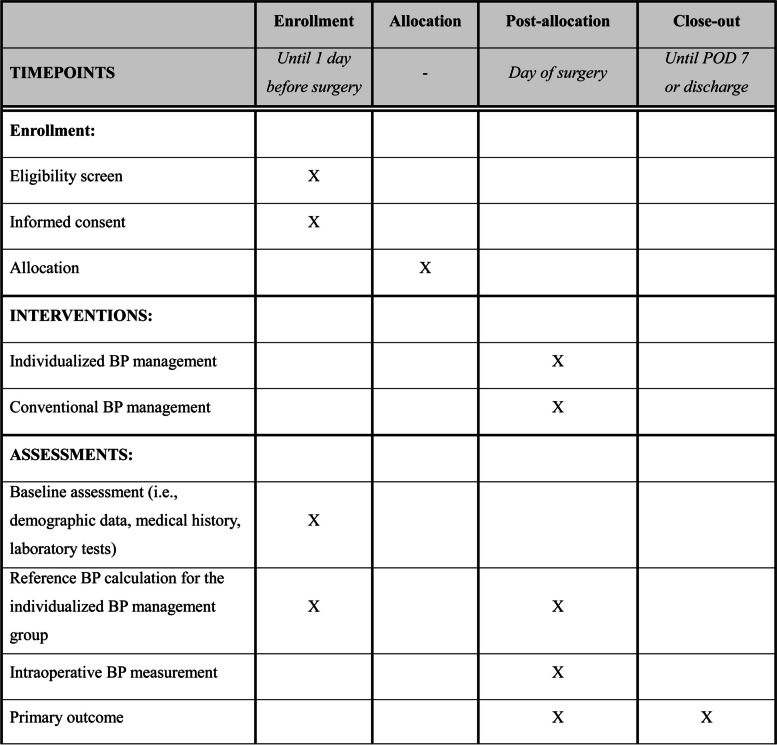
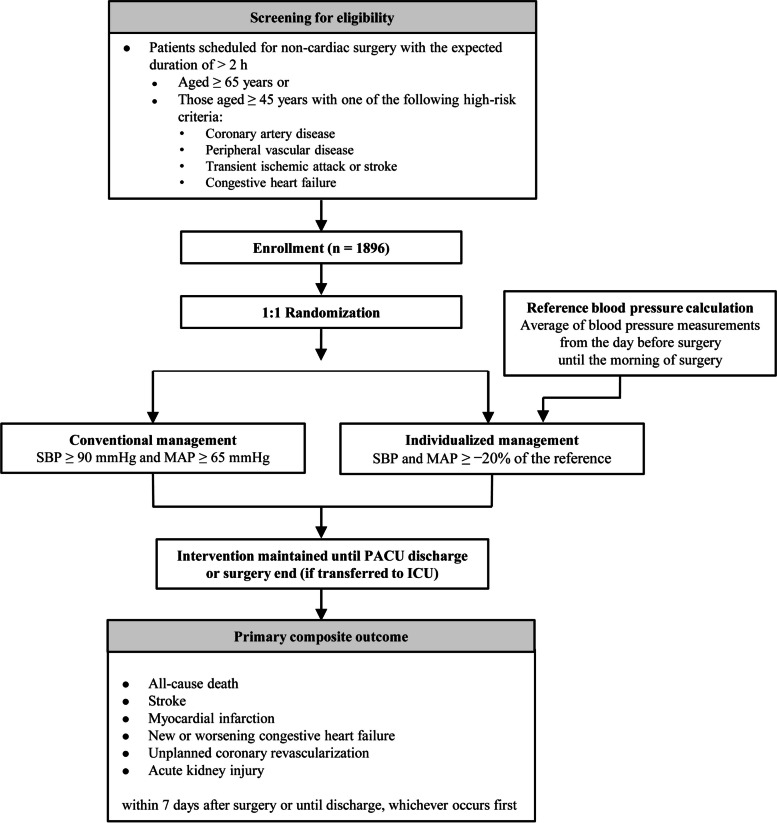
This multicenter, randomized controlled superiority trial will enroll 1896 high-risk patients undergoing major noncardiac surgery from five tertiary university hospitals in South Korea. In the control group, mean arterial pressure will be maintained at ≥ 65 mmHg and systolic blood pressure ≥ 90 mmHg during surgery. In the intervention group, mean arterial pressure and systolic blood pressure will be maintained at no less than 20% of their baseline values. The baseline values are calculated as the average of all values measured from the day before surgery until the morning of surgery. These targets will be maintained until the patient is discharged from the post-anesthesia care unit or, for those who are transferred to the intensive care unit after surgery, until the end of the surgery. No specific restrictions, except for these blood pressure targets, will be applied to perioperative management. The primary composite outcome consists of all-cause death, stroke, myocardial infarction, new or worsening congestive heart failure, unplanned coronary revascularization, and acute kidney injury within 7 days after noncardiac surgery or until hospital discharge, whichever occurs first.
This study will reveal if individualized perioperative blood pressure management decreases the risk of major adverse outcomes in patients at high-risk undergoing noncardiac surgery.
ClinicalTrials.gov NCT06225453. Registered on January 26, 2024.
术中低血压在手术过程中非常常见,并且与主要器官功能障碍和死亡率相关。目前围手术期血压管理很大程度上基于60 - 70mmHg平均动脉压的通用血压阈值。然而,这种传统管理的有效性在前瞻性随机试验中尚未得到证实。因此,我们将开展本研究以测试个体化围手术期血压管理是否能降低术后主要不良结局的发生率。
这项多中心、随机对照优势试验将纳入来自韩国五家三级大学医院的1896例接受非心脏大手术的高危患者。在对照组中,手术期间平均动脉压将维持在≥65mmHg且收缩压≥90mmHg。在干预组中,平均动脉压和收缩压将维持在不低于其基线值的20%。基线值计算为从手术前一天直至手术当天早晨所测所有值的平均值。这些目标将维持至患者从麻醉后护理单元出院,或者对于术后转入重症监护病房的患者,维持至手术结束。除这些血压目标外,围手术期管理不应用特定限制。主要复合结局包括非心脏手术后7天内或直至出院(以先发生者为准)的全因死亡、中风、心肌梗死、新发或加重的充血性心力衰竭、非计划性冠状动脉血运重建以及急性肾损伤。
本研究将揭示个体化围手术期血压管理是否能降低接受非心脏手术的高危患者发生主要不良结局的风险。
ClinicalTrials.gov NCT06225453。于2024年1月26日注册。