Chiba Kiyoshi, Kinebuchi Satoshi, Komagamine Masahide, Tanigawa Kazuyoshi, Chikada Masahide, Nishimaki Hiroshi, Nawata Kan
Department of Cardiovascular Surgery, St Marianna University School of Medicine, Kawasaki, Kanagawa, Japan.
Ann Vasc Dis. 2024 Dec 25;17(4):429-432. doi: 10.3400/avd.cr.24-00099. Epub 2024 Oct 8.
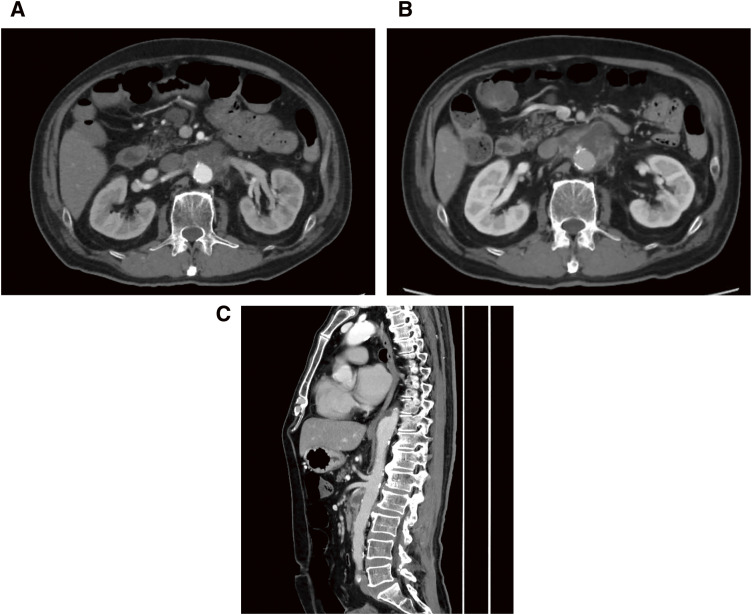
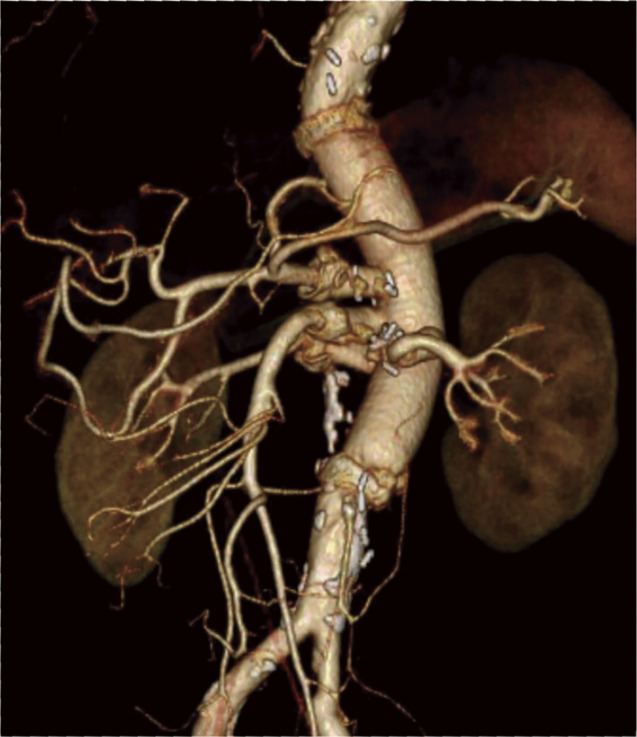
Myasthenia gravis (MG) is an autoimmune neuromuscular junction disorder that rarely coexists with infectious thoracoabdominal aortic aneurysms (TAAA) requiring open repair. A 57-year-old patient with MG underwent elective thoracoabdominal aortic replacement. He was diagnosed with MG (Osserman classification II A). Extent IV thoracoabdominal aortic repair was performed under general anesthesia and maintained by total intravenous anesthesia. The patient was withdrawn from the ventilator on postoperative day 5 without spinal cord ischemia and myasthenic crisis. The management of infectious TAAA with myasthenia gravis warrants not only the prevention of complications associated with the crisis but also multidisciplinary treatments for infection control.
重症肌无力(MG)是一种自身免疫性神经肌肉接头疾病,很少与需要开放修复的感染性胸腹主动脉瘤(TAAA)共存。一名57岁的重症肌无力患者接受了择期胸腹主动脉置换术。他被诊断为重症肌无力(奥斯勒曼分类II A型)。在全身麻醉下进行IV型胸腹主动脉修复,并采用全静脉麻醉维持。患者术后第5天脱离呼吸机,未发生脊髓缺血和重症肌无力危象。重症肌无力合并感染性胸腹主动脉瘤的治疗不仅需要预防与危象相关的并发症,还需要多学科治疗来控制感染。