Alhyari Amjad, Dob Oussama, Safai Zadeh Ehsan, Dietrich Christoph Frank, Trenker Corrina, Gress Thomas M, Görg Christian
Gastroenterology, Endocrinology, Metabolism and Clinical Infectiology, University Hospital Giessen and Marburg, Philipp University of Marburg, Baldingerstraße, 35037 Marburg, Germany.
Interdisciplinary Centre of Ultrasound Diagnostics, University Hospital Giessen and Marburg, Philipp University of Marburg, Baldingerstraße, 35037 Marburg, Germany.
Diseases. 2024 Nov 30;12(12):308. doi: 10.3390/diseases12120308.
To evaluate the ability of acoustic radiation force impulse (ARFI) elastography in differentiating benign from malignant etiologies of splenomegaly based on differences in splenic stiffness.
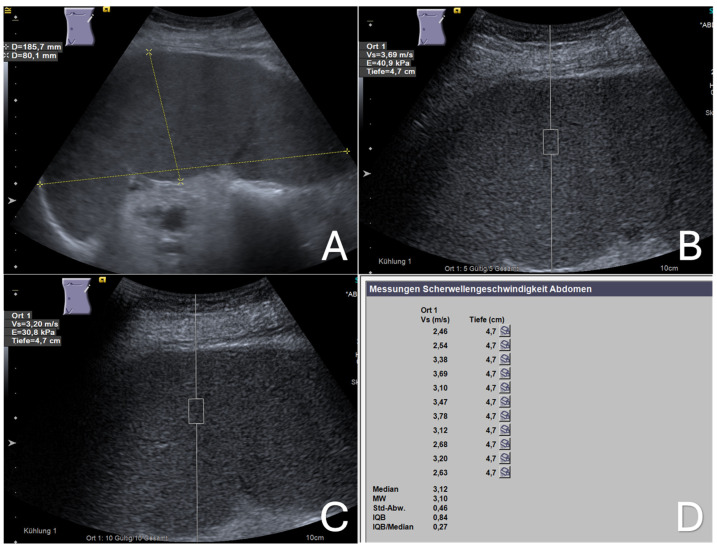
Between September 2020 and November 2022, we evaluated 40 patients with splenomegaly-defined by a splenic long axis greater than 13 cm and/or a short axis greater than 6 cm, without visible focal or infiltrative mass lesions-using abdominal ultrasound at our university hospital. Each patient also underwent a standardized ARFI elastographic assessment of the enlarged spleen, with data collected prospectively. We then retrospectively analyzed the cases with confirmed etiologies of splenomegaly from their final medical reports. Mean ARFI velocities (MAV) were compared across patients with splenomegaly due to malignant infiltration (MIS) from hematological malignancy, congestive splenomegaly (CS) due to portal or splenic vein congestion/occlusion, and immune-related splenomegaly (IRS) associated with systemic infectious or autoimmune diseases.
Among the 40 patients with splenomegaly, 21 (52.5%) were diagnosed with malignant infiltrative splenomegaly (MIS), 11 (27.5%) with congestive splenomegaly (CS), and 8 (20%) with immune-related splenomegaly (IRS). The mean ARFI velocities (MAV) for the MIS, CS, and IRS groups were 3.25 ± 0.68 m/s, 3.52 ± 0.47 m/s, and 2.84 ± 0.92 m/s, respectively. No significant differences were observed in splenic stiffness (MAV) among these groups.
Differentiating between benign and malignant etiologies of splenomegaly based on stiffness differences observed in ARFI elastography is not feasible. Larger prospective studies are necessary to validate these findings.
基于脾脏硬度差异,评估声辐射力脉冲(ARFI)弹性成像在鉴别脾肿大的良性与恶性病因方面的能力。
2020年9月至2022年11月期间,我们在大学医院使用腹部超声对40例脾肿大患者进行了评估,脾肿大定义为脾长轴大于13 cm和/或短轴大于6 cm,且无可见的局灶性或浸润性肿块病变。每位患者还接受了对肿大脾脏的标准化ARFI弹性成像评估,并前瞻性收集数据。然后,我们从最终医学报告中回顾性分析了脾肿大病因已确诊的病例。比较了因血液系统恶性肿瘤导致的恶性浸润性脾肿大(MIS)、因门静脉或脾静脉充血/阻塞导致的充血性脾肿大(CS)以及与全身性感染或自身免疫性疾病相关的免疫相关性脾肿大(IRS)患者的平均ARFI速度(MAV)。
在40例脾肿大患者中,21例(52.5%)被诊断为恶性浸润性脾肿大(MIS),11例(27.5%)为充血性脾肿大(CS),8例(20%)为免疫相关性脾肿大(IRS)。MIS、CS和IRS组的平均ARFI速度(MAV)分别为3.25±0.68 m/s、3.52±0.47 m/s和2.84±0.92 m/s。这些组之间在脾脏硬度(MAV)方面未观察到显著差异。
基于ARFI弹性成像中观察到的硬度差异来鉴别脾肿大的良性与恶性病因是不可行的。需要更大规模的前瞻性研究来验证这些发现。