Fadel Aya, Hussain Hussain, Hernandez Robert J, Clichy Silva Amanda Marie, Estil-Las Amir Agustin, Hamad Mohammad, Saadoon Zahraa F, Naseer Lamia, Sultan William C, Sultan Carla, Schnepp Taylor, Jayakumar Arumugam R
Department of Internal Medicine at Ocean Medical Center, Hackensack Meridian Health, Hackensack, NJ 07601, USA.
Department of Internal Medicine, HCA Florida Kendall Hospital, Miami, FL 33175, USA.
Neurol Int. 2024 Dec 2;16(6):1653-1665. doi: 10.3390/neurolint16060120.
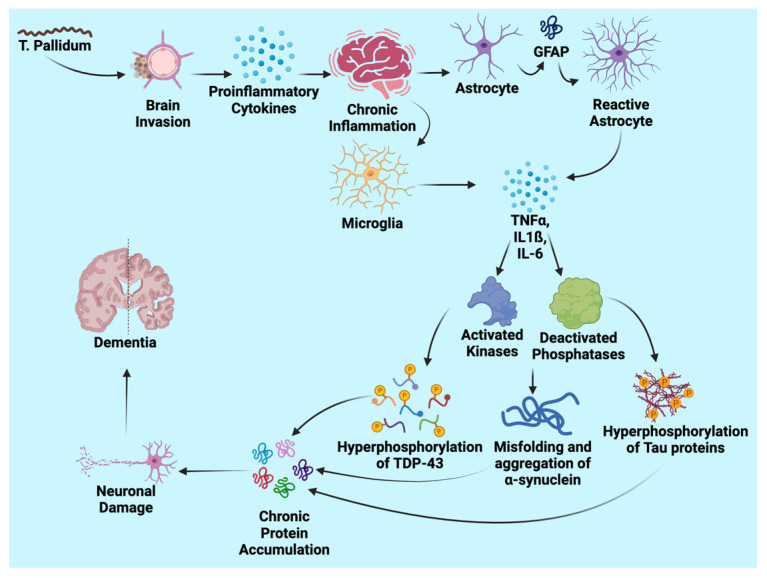
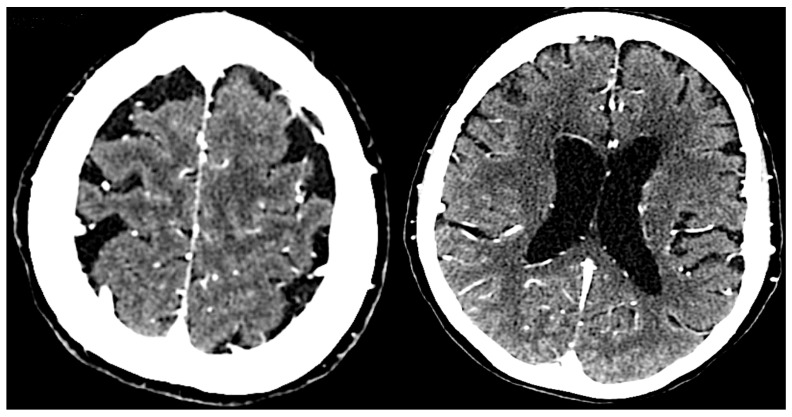
Neurosyphilis-induced dementia represents a severe manifestation of tertiary syphilis, characterized by cognitive and neuropsychiatric impairments. This condition arises from the progression of syphilis to the central nervous system, where the spirochete causes damage through invasion, chronic inflammation, and neurodegeneration. The pathophysiology involves chronic inflammatory responses, direct bacterial damage, and proteinopathies. triggers an inflammatory cascade, resulting in neuronal injury and synaptic dysfunction. Abnormal protein accumulations, including TAR DNA-binding protein 43 (TDP-43) and tau, contribute to neuronal loss and cognitive decline. Seizures, psychiatric symptoms, and motor deficits further complicate the progression of dementia. Diagnosis includes clinical assessment, cerebrospinal fluid analysis, and neuroimaging. Diagnostic tests include CSF-VDRL, FTA-ABS, and neuroimaging techniques such as MRI and PET scans, which help detect structural changes and confirm neurosyphilis. Management of neurosyphilis-induced dementia involves antibiotic therapy and psychotropic medications to address both infectious and symptomatic components. While penicillin remains the cornerstone of treatment, psychotropic agents, including haloperidol, risperidone, quetiapine, and divalproex sodium, can manage psychiatric symptoms. However, careful monitoring is required due to potential side effects and interactions with ongoing treatment. Overall, early diagnosis and comprehensive management are crucial for mitigating the cognitive and neuropsychiatric impairments associated with neurosyphilis-induced dementia.
神经梅毒所致痴呆是三期梅毒的一种严重表现,其特征为认知和神经精神障碍。这种情况源于梅毒进展至中枢神经系统,螺旋体通过侵袭、慢性炎症和神经退行性变造成损害。病理生理学涉及慢性炎症反应、细菌直接损伤和蛋白病。引发炎症级联反应,导致神经元损伤和突触功能障碍。异常蛋白质积聚,包括TAR DNA结合蛋白43(TDP - 43)和tau蛋白,会导致神经元丢失和认知衰退。癫痫发作、精神症状和运动功能障碍使痴呆的进展更加复杂。诊断包括临床评估、脑脊液分析和神经影像学检查。诊断测试包括脑脊液性病研究实验室玻片试验(CSF - VDRL)、荧光螺旋体抗体吸收试验(FTA - ABS)以及MRI和PET扫描等神经影像学技术,这些有助于检测结构变化并确诊神经梅毒。神经梅毒所致痴呆的治疗包括抗生素治疗和精神药物治疗,以解决感染性和症状性成分。虽然青霉素仍然是治疗的基石,但包括氟哌啶醇、利培酮、喹硫平和丙戊酸钠在内的精神药物可以控制精神症状。然而,由于潜在的副作用以及与正在进行的治疗的相互作用,需要仔细监测。总体而言,早期诊断和综合管理对于减轻与神经梅毒所致痴呆相关的认知和神经精神障碍至关重要。