Lim Yee Cherng, Hamdan Mukhri, Maheshwari Abha, Cheong Ying
Complete Fertility, Princess Anne Hospital, Level F, Coxford Road, Southampton, SO16 5YA, UK.
Department of Obstetrics and Gynaecology, Universiti Malaya, 50603, Kuala Lumpur, Malaysia.
Sci Rep. 2024 Dec 28;14(1):30826. doi: 10.1038/s41598-024-81539-z.
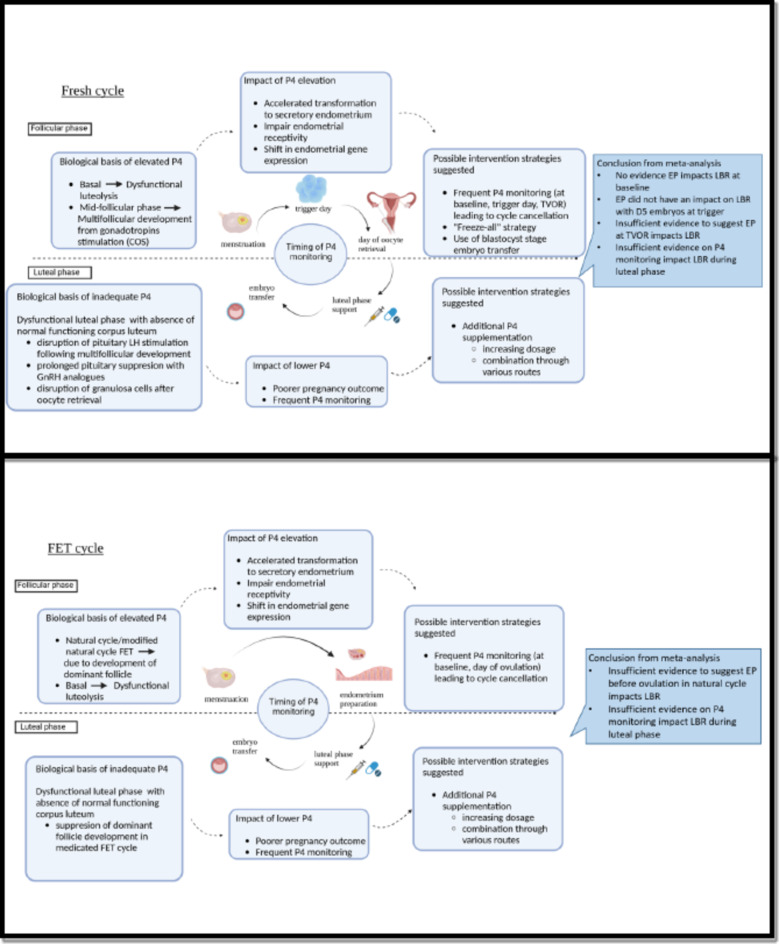
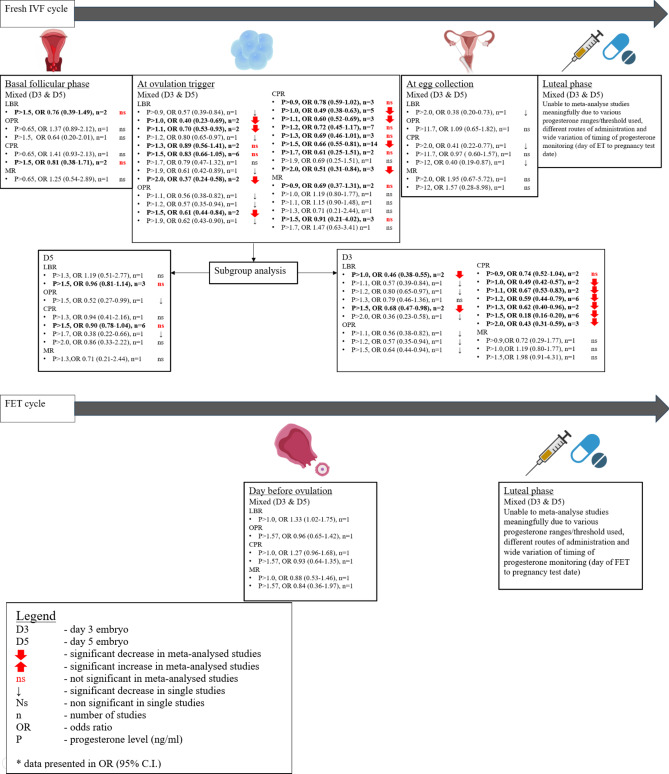
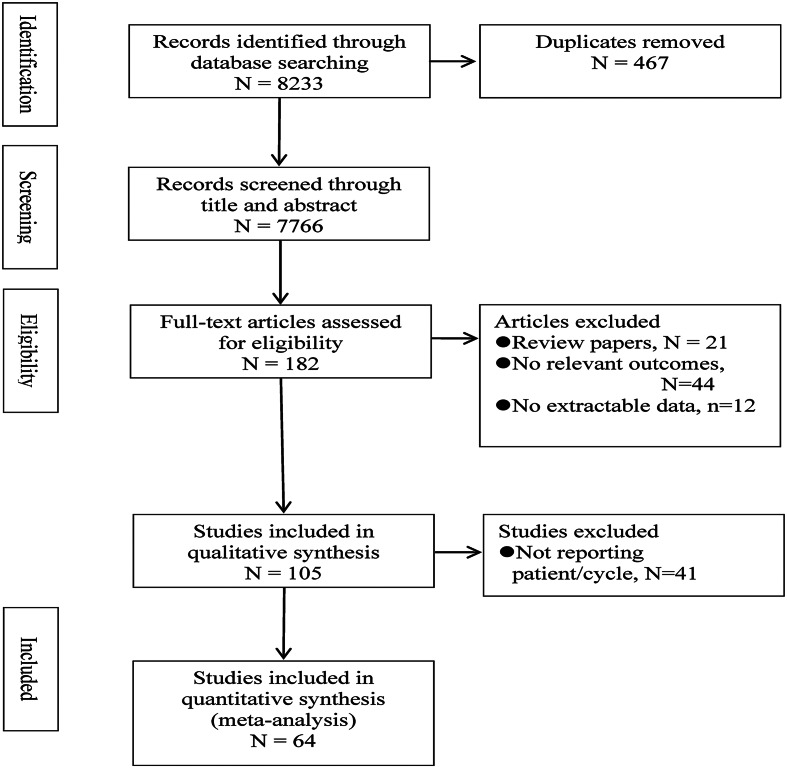
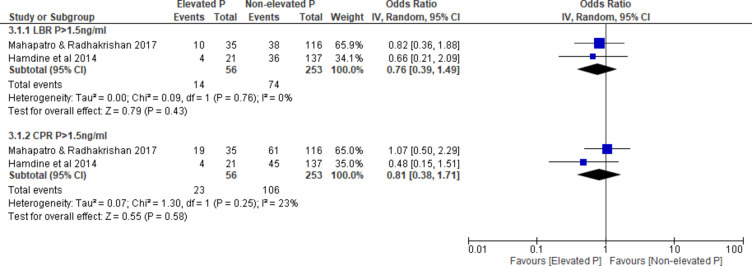
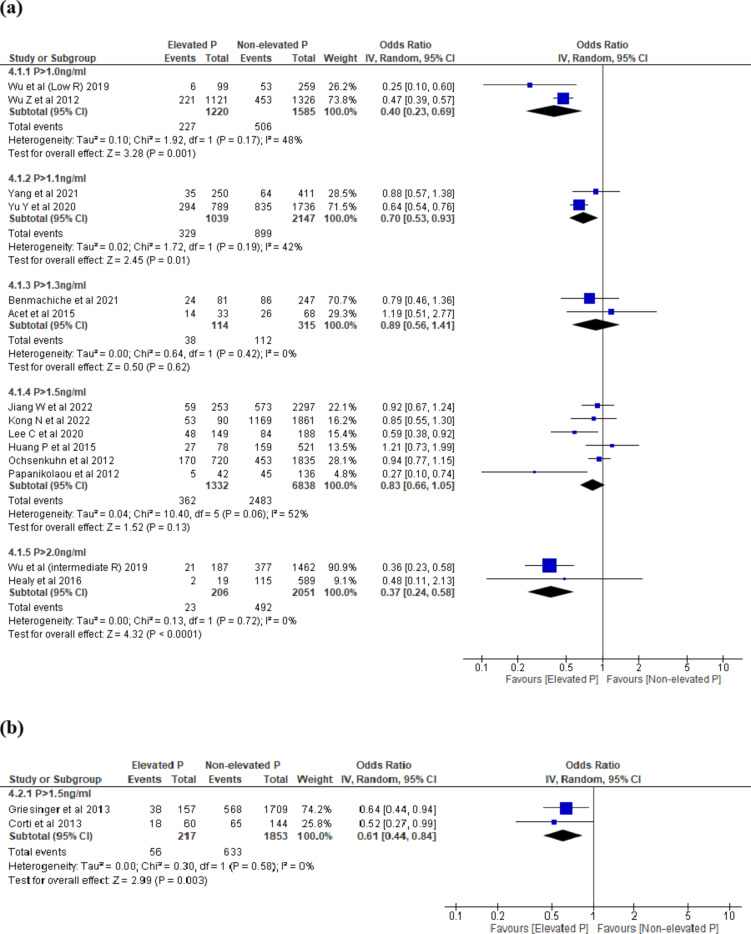
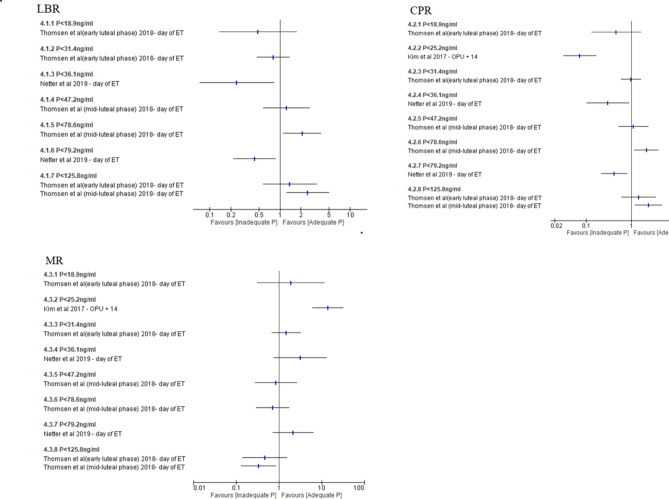
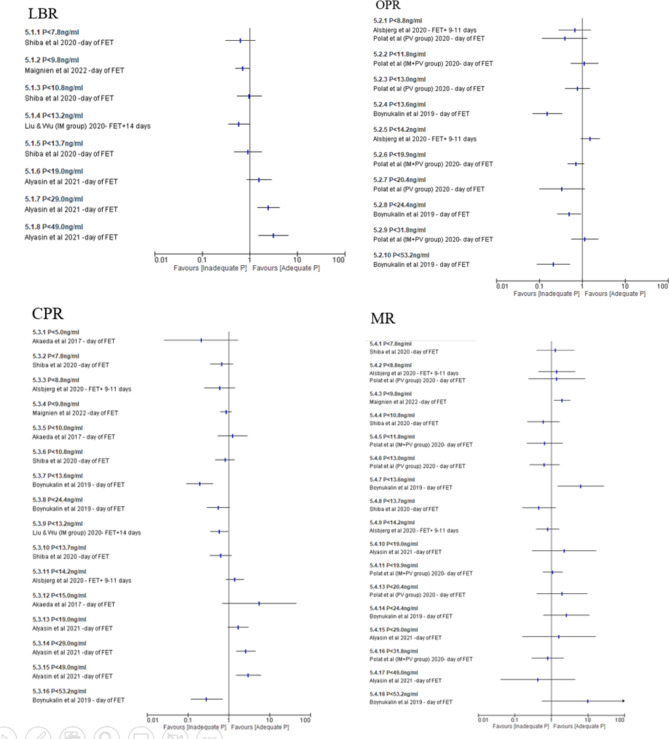
Elevated progesterone (EP) or inadequate progesterone levels during ART cycle monitoring may lead to cycle cancellations or further progesterone supplementation, but practice varies. It remains controversial whether modifying clinical practice in the presence or absence of EP improves clinical outcomes. This systematic review aims to investigate if progesterone levels at different phases of fresh and frozen ART cycles influence pregnancy outcomes, in particular, that pertaining to day 3 versus day 5 embryo transfers. A systematic search of EMBASE, MEDLINE, CINAHL, PubMed, SCOPUS and Web of Science identified studies from the year 2000. We included studies with women undergoing fresh and frozen IVF/ICSI cycles; with extractable per woman data on pregnancy outcomes where serum progesterone measurement was performed. We excluded interventional studies that influence clinical decisions or studies with donor cycles. The Newcastle Ottawa Scale (NOS) was used to determine the risk of bias. The primary outcome was LBR, and the secondary outcomes were OPR, CPR and MR. PICOS study protocol was used to include non-randomized studies of interventions (NRSI). Analysis was done using RevMan5 and the studies were pooled using the DerSimonian and Laird for random effects meta-analysis. The study was registered with PROSPERO (registration ID CRD42022382423). 64 studies (N = 57,988 women) were included. In fresh cycles, there is no evidence that at baseline EP impacts LBR (P > 1.5 ng/ml, OR 0.76 [95% CI 0.39-1.49], 2 studies, N = 309) and CPR (P > 1.5 ng/ml, OR 0.81 [0.38-1.71], 2 studies, N = 309). EP at ovulation trigger is associated with a lower LBR (P > 1.0 ng/ml, OR 0.40 [0.23-0.69], 2 studies, N = 2805) and CPR (P > 1.0 ng/ml, OR 0.49 [0.42-0.58], 3 studies, N = 3323; P > 1.1 ng/ml, OR 0.66 [0.53-0.83], 2 studies, N = 2444; P > 1.2 ng/ml, OR 0.61 [0.39-0.96], 6 studies, N = 844; P > 1.5 ng/ml, OR 0.37 [0.17-0.81], 6 studies, N = 13,870; P > 2.0 ng/ml, OR 0.43 [0.31-0.59], 3 studies, N = 1949) with D3 embryo but not D5 [LBR (P > 1.5 ng/ml, OR 1.02 [0.74-1.39], 3 studies, N = 5174) and CPR (P > 1.5 ng/ml, OR 0.88 [0.67-1.14], 6 studies, N = 5705)]. We could not meaningfully meta-analyse studies on the day of egg collection in fresh cycles, embryo transfer in fresh cycles, at ovulation trigger or before ovulation in natural FET cycles and FET cycles due to significant study heterogeneity. We acknowledged the limitations on including studies post year 2000 and the exclusion of studies with multiple observations, which may result in inherent publication bias and some confounding factors uncontrolled for. In conclusion, in controlled ovarian stimulation, EP at baseline did not impact on LBR; EP at ovulation trigger is associated with a lower LBR for D3 but not for D5 embryo transfer. In FET cycles, as the studies were heterogeneous, we were unable to combine the data in a meaningful way. This review is sponsored by Complete Fertility and the Ministry of Health, Malaysia.
在辅助生殖技术(ART)周期监测期间,孕酮水平升高(EP)或孕酮水平不足可能导致周期取消或进一步补充孕酮,但实践情况各不相同。在有或没有EP的情况下改变临床实践是否能改善临床结局仍存在争议。本系统评价旨在研究新鲜和冷冻ART周期不同阶段的孕酮水平是否会影响妊娠结局,特别是与第3天和第5天胚胎移植相关的结局。对EMBASE、MEDLINE、CINAHL、PubMed、SCOPUS和Web of Science进行系统检索,确定了2000年以来的研究。我们纳入了接受新鲜和冷冻体外受精/卵胞浆内单精子注射(IVF/ICSI)周期的女性的研究;有每位女性关于妊娠结局的可提取数据,且进行了血清孕酮测量。我们排除了影响临床决策的干预性研究或供体周期的研究。使用纽卡斯尔渥太华量表(NOS)来确定偏倚风险。主要结局是活产率(LBR),次要结局是着床率(OPR)、临床妊娠率(CPR)和流产率(MR)。使用PICOS研究方案纳入干预性非随机研究(NRSI)。使用RevMan5进行分析,并使用DerSimonian和Laird方法进行随机效应荟萃分析对研究进行汇总。该研究已在国际前瞻性系统评价注册库(PROSPERO)注册(注册号CRD42022382423)。纳入了64项研究(N = 57988名女性)。在新鲜周期中,没有证据表明基线时的EP会影响LBR(P > 1.5 ng/ml,比值比[OR] 0.76 [95%置信区间(CI)0.39 - 1.49],2项研究,N = 309)和CPR(P > 1.5 ng/ml,OR 0.81 [0.38 - 1.71],2项研究,N = 309)。触发排卵时的EP与较低的LBR相关(P > 1.0 ng/ml,OR 0.40 [0.23 - 0.69],2项研究,N = 2805)和CPR(P > 1.0 ng/ml,OR 0.49 [0.42 - 0.58],3项研究,N = 3323;P > 1.1 ng/ml,OR 0.66 [0.53 - 0.83],2项研究,N = 2444;P > 1.2 ng/ml,OR 0.61 [0.39 - 0.96],6项研究,N = 844;P > 1.5 ng/ml,OR 0.37 [0.17 - 0.81],6项研究,N = 13870;P > 2.0 ng/ml,OR 0.43 [0.31 - 0.59],3项研究,N = 1949),对于第3天胚胎移植是这样,但第5天胚胎移植并非如此[LBR(P > 1.5 ng/ml,OR 1.02 [0.74 - 1.39],3项研究,N = 5174)和CPR(P > 1.5 ng/ml,OR 0.88 [0.67 - 1.14],6项研究,N = 5705)]。由于显著的研究异质性,我们无法对新鲜周期取卵日、新鲜周期胚胎移植日、自然冷冻胚胎移植(FET)周期触发排卵时或排卵前以及FET周期的研究进行有意义的荟萃分析。我们承认纳入2000年以后的研究以及排除有多次观察结果的研究存在局限性,这可能导致内在的发表偏倚以及一些未控制的混杂因素。总之,在控制性卵巢刺激中,基线时的EP不影响LBR;触发排卵时的EP与第3天胚胎移植的较低LBR相关,但与第5天胚胎移植无关。在FET周期中,由于研究具有异质性,我们无法以有意义的方式合并数据。本综述由马来西亚全生育中心和卫生部赞助。