Mao Chenyu, Xiong Anwen, Qian Jiong, Wang Wenxiang, Liu Ying, Zhang Tao, Wu Zhihai, Ni Haiqing, Lu Jia, Long Sixiang, Zhao Li, Chen Yuling, Zhou Caicun, Xu Nong
The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China.
Shanghai East Hospital, Tongji University School of Medicine, Shanghai, China.
J Hematol Oncol. 2024 Dec 31;17(1):132. doi: 10.1186/s13045-024-01651-5.
Co-inhibition of immune checkpoints lymphocyte-activation gene 3 (LAG-3) and PD-1 is believed to enhance cancer immunotherapy through synergistic effects. Herein, we evaluate the safety and efficacy of IBI110 (anti-LAG-3 antibody) with sintilimab (an anti-PD-1 antibody) in Chinese patients with advanced solid tumors.
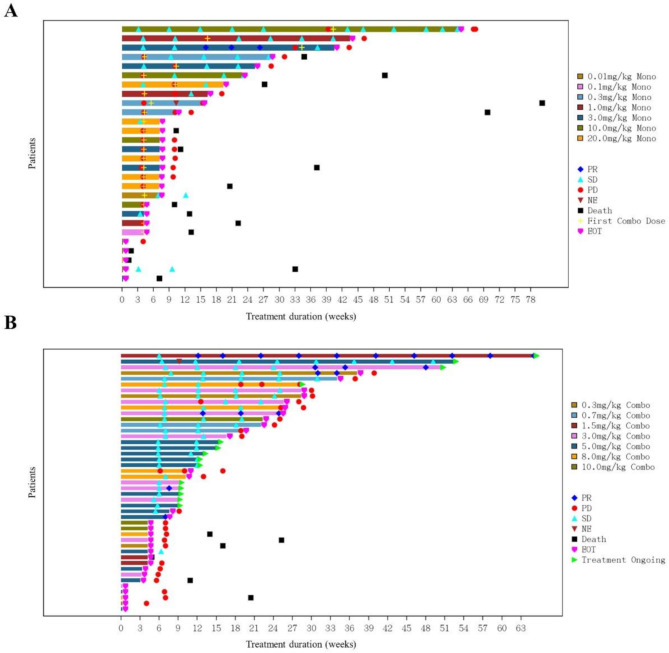
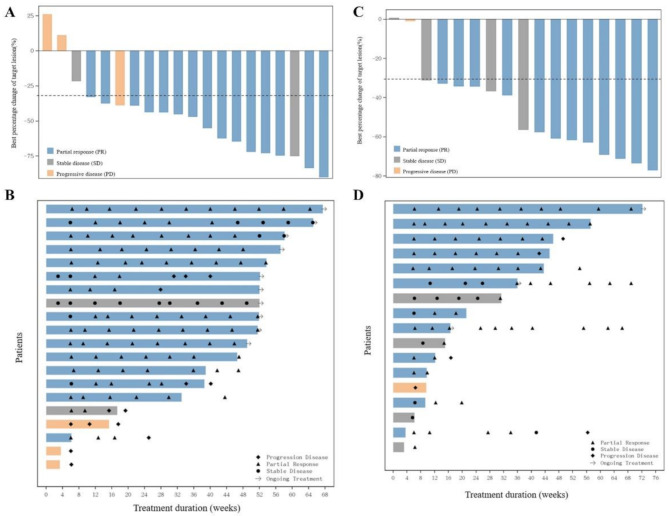
In this open-label phase I study, phase Ia dose escalation of IBI110 monotherapy and phase Ib combination dose escalation of IBI110 plus sintilimab were conducted in patients with advanced solid tumors. Additionally, phase Ib combination dose expansion of IBI110 plus sintilimab and chemotherapy was conducted in previously untreated, advanced squamous non-small cell lung cancer (sqNSCLC) and HER-2 negative gastric cancer (GC). In phase Ia dose escalation, patients received IBI110 monotherapy at 0.01/0.1/0.3/1/3/10/20 mg/kg Q3W. In phase Ib dose escalation, patients received IBI110 at 0.3/0.7/1.5/3/5/8/10 mg/kg Q3W plus sintilimab 200 mg Q3W. In phase Ib combination dose expansion, patients received IBI110 at recommended phase 2 dose (RP2D) plus sintilimab 200 mg Q3W and chemotherapy. The primary endpoints were safety, tolerability and efficacy including objective response rate (ORR), disease control rate (DCR), duration of response (DoR), progression-free survival (PFS) assessed by RECIST v1.1 and overall survival (OS). The secondary endpoints included pharmacokinetics, pharmacodynamics and immunogenicity.
In phase Ia dose escalation (n = 28), treatment-related adverse events (TRAEs) occurred in 67.9% patients and grade ≥ 3 TRAEs occurred in 21.4% patients. In phase Ib combination dose escalation (n = 45), TRAEs occurred in 75.6% patients and grade ≥ 3 TRAEs occurred in 22.2% patients. No dose-limiting toxicity (DLT) was observed. The most common TRAE was anemia (17.9%, including 3.6% ≥ G3) in phase Ia dose escalation of IBI110 monotherapy (n = 28), aspartate aminotransferase increased (28.9%, all G1-G2) in phase Ib dose escalation of IBI110 plus sintilimab (n = 45), anemia (70.0%, all G1-G2) in phase Ib dose expansion in sqNSCLC (n = 20), and neutrophil count decreased (64.7%, including 17.6%≥ G3) in phase Ib dose expansion in GC (n = 17). The RP2D of IBI110 was determined at 200 mg (3 mg/kg) Q3W. ORR in phase Ia/Ib dose escalation was 3.6% with IBI110 monotherapy and 14% with IBI110 plus sintilimab. In phase Ib combination dose expansion of IBI110 plus sintilimab and chemotherapy, unconfirmed and confirmed ORR in sqNSCLC (n = 20) was 80.0% (95% CI, 56.3-94.3) and 75.0% (95% CI, 50.9-91.3), respectively and in GC (n = 17) was 88.2% (95% CI, 63.6-98.5) and 70.6% (95% CI, 44.0-89.7), respectively.
IBI110 monotherapy and in combination with sintilimab were well-tolerated in Chinese patients with advanced solid tumors. Encouraging efficacy of IBI110 in combination with sintilimab and chemotherapies was observed in sqNSCLC and GC.
ClinicalTrials.gov Identifier: NCT04085185.
免疫检查点淋巴细胞激活基因3(LAG-3)和程序性死亡受体1(PD-1)的联合抑制被认为可通过协同效应增强癌症免疫治疗。在此,我们评估IBI110(抗LAG-3抗体)联合信迪利单抗(一种抗PD-1抗体)在中国晚期实体瘤患者中的安全性和疗效。
在这项开放标签的I期研究中,对晚期实体瘤患者进行了IBI110单药治疗的Ia期剂量递增以及IBI110联合信迪利单抗的Ib期联合剂量递增。此外,在先前未治疗的晚期鳞状非小细胞肺癌(sqNSCLC)和人表皮生长因子受体2(HER-2)阴性胃癌(GC)患者中进行了IBI110联合信迪利单抗及化疗的Ib期联合剂量扩展。在Ia期剂量递增阶段,患者接受0.01/0.1/0.3/1/3/10/20 mg/kg的IBI110单药治疗,每3周一次(Q3W)。在Ib期剂量递增阶段,患者接受0.3/0.7/1.5/3/5/8/10 mg/kg Q3W的IBI110联合200 mg Q3W的信迪利单抗治疗。在Ib期联合剂量扩展阶段,患者接受推荐的2期剂量(RP2D)的IBI110联合200 mg Q3W的信迪利单抗及化疗。主要终点为安全性、耐受性和疗效,包括客观缓解率(ORR)、疾病控制率(DCR)、缓解持续时间(DoR)、根据实体瘤疗效评价标准(RECIST)v1.1评估的无进展生存期(PFS)和总生存期(OS)。次要终点包括药代动力学、药效学和免疫原性。
在Ia期剂量递增阶段(n = 28),67.9%的患者发生了治疗相关不良事件(TRAEs),21.4%的患者发生了≥3级TRAEs。在Ib期联合剂量递增阶段(n = 45),75.6%的患者发生了TRAEs,22.2%的患者发生了≥3级TRAEs。未观察到剂量限制毒性(DLT)。在IBI110单药治疗的Ia期剂量递增阶段(n = 28),最常见的TRAEs是贫血(17.9%,包括3.6%的≥3级);在IBI110联合信迪利单抗的Ib期剂量递增阶段(n = 45),是天冬氨酸转氨酶升高(28.9%,均为1-2级);在sqNSCLC的Ib期剂量扩展阶段(n = 20),是贫血(70.0%,均为1-2级);在GC的Ib期剂量扩展阶段(n = 17),是中性粒细胞计数降低(64.7%,包括17.6%的≥3级)。IBI110的RP2D确定为200 mg(3 mg/kg)Q3W。在Ia/Ib期剂量递增阶段,IBI110单药治疗的ORR为3.6%,IBI110联合信迪利单抗的ORR为14%。在IBI110联合信迪利单抗及化疗的Ib期联合剂量扩展阶段,sqNSCLC(n = 20)中未经确认和确认的ORR分别为80.0%(95%CI,56.3-94.3)和75.0%(95%CI,50.9-91.3),GC(n = 17)中分别为88.2%(95%CI,63.6-98.5)和70.6%(95%CI,44.0-89.7)。
IBI110单药治疗及联合信迪利单抗在中国晚期实体瘤患者中耐受性良好。在sqNSCLC和GC中观察到IBI110联合信迪利单抗及化疗具有令人鼓舞的疗效。
ClinicalTrials.gov标识符:NCT04085185。