Gupta Abha A, Tinker Anna, Jonker Derek, Jamal Rahma, Hirte Hal, Winquist Eric W, Chu Quincy, Kollmannsberger Christian, Wong Ralph, Alcindor Thierry, Nielsen Torsten O, Tsao Ming, Cottrell Tricia R, Provencher Diane, Hilton John, Krzyżanowska Monika K, Elser Christine, Hotte Sebastien, Sederias Joana, Zhang Siwei, Tu Wei, Dancey Janet
University Health Network, Princess Margaret Cancer Centre, Toronto, ON, Canada.
CAVA - BCCA - Vancouver, BC, Canada.
EClinicalMedicine. 2024 Dec 10;79:102991. doi: 10.1016/j.eclinm.2024.102991. eCollection 2025 Jan.
Dual inhibition of cytotoxic T-lymphocyte associated protein 4 (CTLA-4) and programmed death ligand 1 (PD-L1) has been shown to be an effective treatment strategy in many cancers. We sought to determine the objective response rate of combination durvalumab (D) plus tremelimumab (TM) in parallel cohorts of patients with carefully selected rare cancer types in which these agents had not previously been evaluated in phase II trials and for which there was clinical or biological rationale for dual immune checkpoint inhibitor therapy to be active.
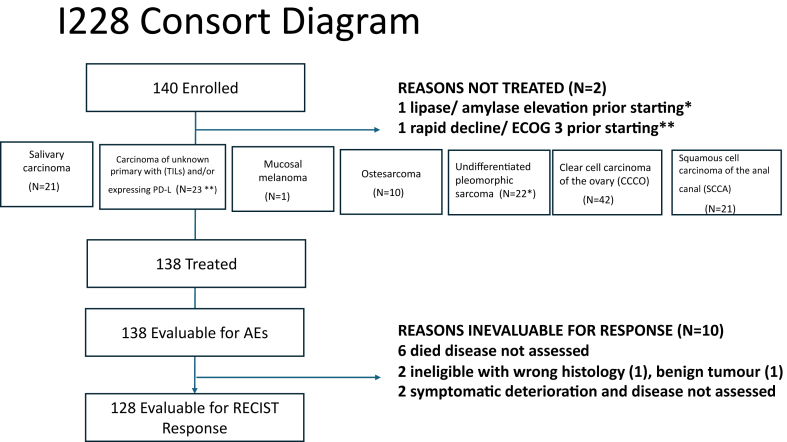
We designed a multi-centre, non-blinded, open-label phase II basket trial with each of the following 8 rare cancers considered a separate phase II trial: salivary carcinoma, carcinoma of unknown primary (CUP) with tumour infiltrating lymphocytes and/or expressing PD-L1, mucosal melanoma, acral melanoma, osteosarcoma, undifferentiated pleomorphic sarcoma, clear cell carcinoma of the ovary (CCCO) or squamous cell carcinoma of the anal canal (SCCA). The primary objective was to evaluate the response rate of the combination of D and TM, and the secondary objectives were to evaluate the tolerability and safety of D and TM combination. Eligible patients had advanced, metastatic or recurrent, or unresectable cancer with no known life-prolonging treatment option, age ≥16 years, ECOG performance status 0 or 1. Patients received D (1500 mg IV) + TM (75 mg IV) on Day 1 q4 weeks for 4 cycles followed by D q4 weeks until disease progression. This trial is registered with ClinicalTrials.gov, NCT02879162.
From December 14th, 2016, to August 14, 2019, 140 patients enrolled into seven cohorts. The rare melanoma cohorts were closed due to lack of accrual. Of the 140 patients enrolled, 138 were eligible, 138 were evaluable for toxicity and 128 (91%) were evaluable for response. Durable responses were noted in all cohorts except for osteosarcoma. The overall response rate for eligible patients was 16% (95% CI: 10-23%). The response rates in each cancer cohort were undifferentiated pleomorphic sarcoma 15% (n = 3/20; 95% CI 3-38%), salivary carcinoma 20% (n = 4/20; 95% CI: 6-44%), CUP 17% (n = 3/18; 95% CI 4-41%), SCCA 10% (n = 2/20; 95% CI 12-32%) and CCCO 21% (n = 8/39; 95% CI 9-37%). Grade 3/4 adverse events were rare, where 4 patients experienced grade 4 related events and39 patients experienced grade 3 events.
Durvalumab + tremelimumab treatment resulted in meaningful responses in salivary carcinoma and CCCO and deserves further exploration in front-line studies.
AstraZeneca and Canadian Cancer Society.
细胞毒性T淋巴细胞相关蛋白4(CTLA-4)和程序性死亡配体1(PD-L1)的双重抑制已被证明是许多癌症的有效治疗策略。我们试图确定度伐利尤单抗(D)联合曲美木单抗(TM)在精心挑选的罕见癌症类型平行队列中的客观缓解率,这些癌症类型此前未在II期试验中进行评估,且有临床或生物学依据表明双重免疫检查点抑制剂治疗可能有效。
我们设计了一项多中心、非盲、开放标签的II期篮子试验,以下8种罕见癌症中的每一种都被视为一项单独的II期试验:唾液腺癌、伴有肿瘤浸润淋巴细胞和/或表达PD-L1的原发灶不明癌(CUP)、黏膜黑色素瘤、肢端黑色素瘤、骨肉瘤、未分化多形性肉瘤、卵巢透明细胞癌(CCCO)或肛管鳞状细胞癌(SCCA)。主要目标是评估D和TM联合治疗的缓解率,次要目标是评估D和TM联合治疗的耐受性和安全性。符合条件的患者患有晚期、转移性或复发性、或不可切除的癌症,且没有已知的延长生命的治疗选择,年龄≥16岁,东部肿瘤协作组(ECOG)体能状态为0或1。患者在第1天接受D(1500mg静脉注射)+TM(75mg静脉注射),每4周一次,共4个周期,随后每4周接受一次D,直至疾病进展。本试验已在ClinicalTrials.gov注册,注册号为NCT02879162。
从2016年12月14日至2019年8月14日,140例患者入组7个队列。罕见黑色素瘤队列因入组不足而关闭。在入组的140例患者中,138例符合条件,138例可评估毒性,128例(91%)可评估缓解情况。除骨肉瘤外,所有队列均观察到持久缓解。符合条件患者的总缓解率为16%(95%CI:10-23%)。各癌症队列的缓解率分别为:未分化多形性肉瘤15%(n = 3/20;95%CI 3-38%)、唾液腺癌20%(n = 4/20;95%CI:6-44%)、CUP 17%(n = 3/18;95%CI 4-41%)、SCCA 10%(n = 2/20;95%CI 1-32%)和CCCO 21%(n = 8/39;95%CI 9-37%)。3/4级不良事件罕见,4例患者发生4级相关事件,39例患者发生3级事件。
度伐利尤单抗+曲美木单抗治疗在唾液腺癌和CCCO中产生了有意义的缓解,值得在一线研究中进一步探索。
阿斯利康和加拿大癌症协会。