Hart Einar A, Braithwaite S A, Hermens J A J, Kraaijeveld A O, Ramjankhan F, van Laake L W, Oerlemans M I F J, Szymanski M K
Department of Cardiology, University Medical Center Utrecht, Utrecht, Netherlands.
Department of Anesthesiology, University Medical Center Utrecht, Utrecht, Netherlands.
Clin Transplant. 2025 Jan;39(1):e70066. doi: 10.1111/ctr.70066.
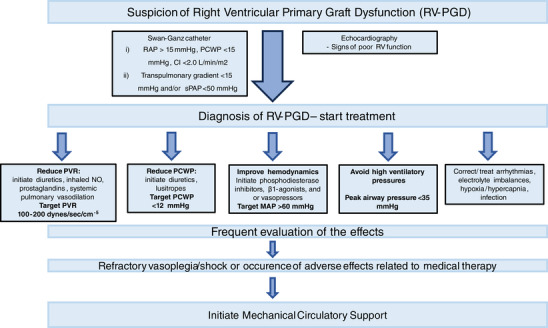
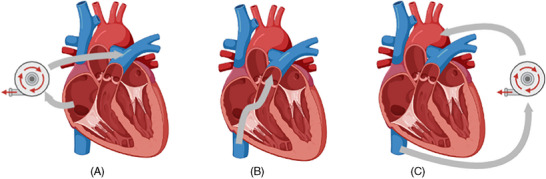
Primary graft dysfunction (PGD) is the most common cause of early mortality following heart transplantation. Although PGD can affect both ventricles, isolated right ventricular dysfunction (RV-PGD) is observed in nearly half of PGD patients. RV-PGD requires specific medical management to support the preload, afterload, and function of the failing RV; however, the use of mechanical circulatory support of the RV (RV-MCS) might be required when optimal medical therapy is insufficient in preventing forward failure and retrograde venous congestion. While RV-MCS options provide the opportunity to prevent or to recover from circulatory shock states, MCS is associated with a significant risk of complications. As a result of recent developments in short-term mechanical support devices, less invasive, percutaneous options for RV-MCS are available. In this review, we discuss the available devices, their advantages and disadvantages, and reported outcomes in RV-PGD.
原发性移植功能障碍(PGD)是心脏移植后早期死亡的最常见原因。尽管PGD可累及双心室,但近半数PGD患者会出现孤立性右心室功能障碍(RV-PGD)。RV-PGD需要特定的药物治疗来维持衰竭右心室的前负荷、后负荷及功能;然而,当最佳药物治疗不足以预防前向性衰竭和逆行性静脉淤血时,可能需要使用右心室机械循环支持(RV-MCS)。虽然RV-MCS可提供预防循环休克状态或从中恢复的机会,但MCS会带来显著的并发症风险。由于短期机械支持装置的最新进展,现在有了侵入性较小的经皮RV-MCS选项。在本综述中,我们讨论了可用的装置、它们的优缺点以及在RV-PGD中的报道结果。