Sato Ryota, Hasegawa Daisuke, Guo Stephanie, Nuqali Abdulelah E, Moreno Jesus E Pino
Division of Critical Care Medicine, Department of Medicine, The Queen's Medical Center, Honolulu, HI, USA.
Division of Pulmonary, Allergy, and Critical Care, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, USA.
J Intensive Care. 2025 Jan 2;13(1):1. doi: 10.1186/s40560-024-00770-y.
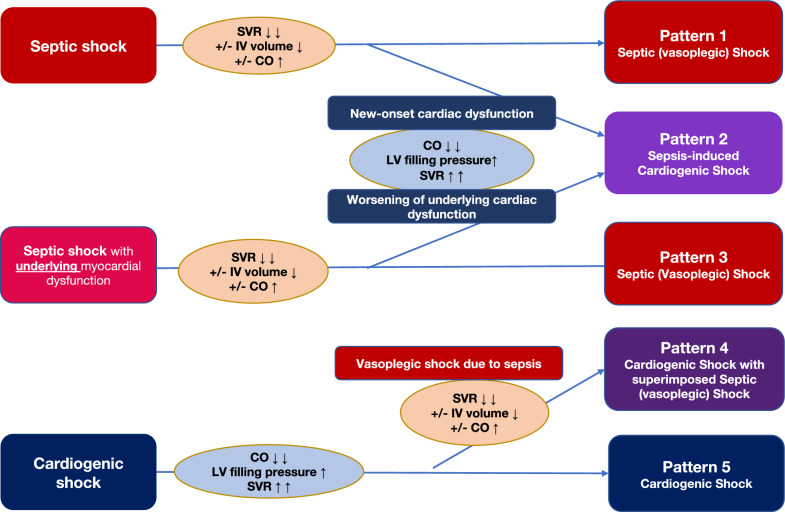
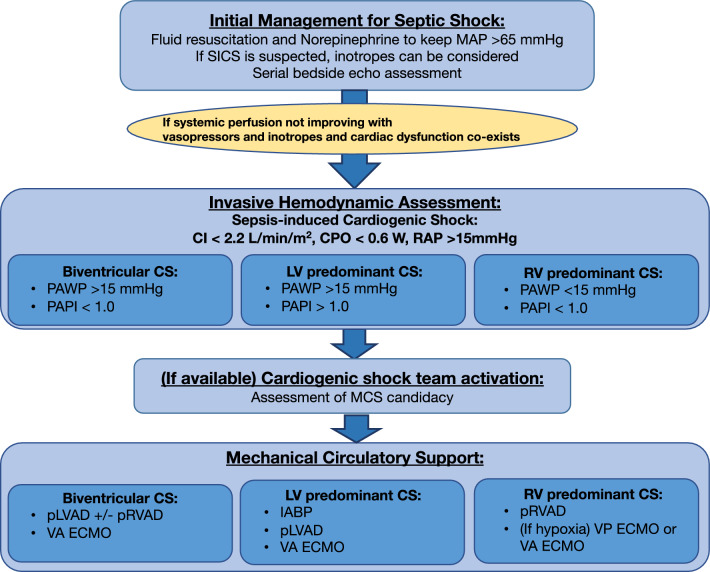
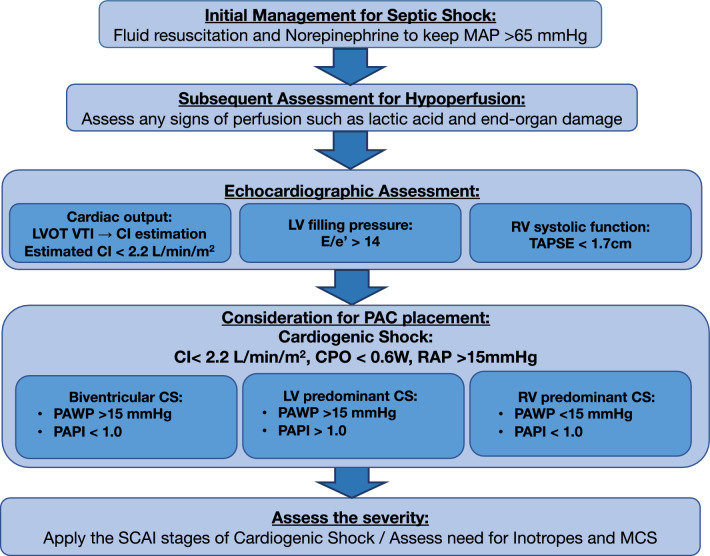
Sepsis often leads to vasoplegia and a hyperdynamic cardiac state, with treatment focused on restoring vascular tone. However, sepsis can also cause reversible myocardial dysfunction, particularly in the elderly with pre-existing heart conditions. The Surviving Sepsis Campaign Guidelines recommend using dobutamine with norepinephrine or epinephrine alone for patients with septic shock with cardiac dysfunction and persistent hypoperfusion despite adequate fluid resuscitation and stable blood pressure. However, the definition of cardiac dysfunction and hypoperfusion in these guidelines remains controversial, leading to varied clinical interpretations. Cardiac dysfunction with persistent hypoperfusion despite restoring adequate preload and afterload is often considered a cardiogenic shock. Therefore, sepsis complicated by new-onset myocardial dysfunction or worsening of underlying myocardial dysfunction due to sepsis-induced cardiomyopathy, resulting in cardiogenic shock, can be defined as "Sepsis-induced cardiogenic shock (SICS)". SICS is known to be associated with significantly higher mortality. A history of cardiac dysfunction is a strong predictor of SICS, highlighting the need for precise diagnosis and management given the aging population and rising cardiovascular disease prevalence. Therefore, SICS might benefit from early invasive hemodynamic monitoring with a pulmonary artery catheter (PAC), unlike those with septic shock alone. While routine PAC monitoring for all septic patients is impractical, echocardiography could be a useful screening tool for high-risk individuals. If echocardiography indicates cardiogenic shock, PAC might be warranted for continuous monitoring. The role of inotropes in SICS remains uncertain. Mechanical circulatory support (MCS) might be considered for severe cases, as high-dose vasopressors and inotropes are associated with worse outcomes. Correct patient selection is the key to improving outcomes with MCS. Engaging a cardiogenic shock team for a multidisciplinary approach can be beneficial. In summary, addressing the evidence gaps in SICS diagnosis and management is crucial. Echocardiography for screening, advanced monitoring with PAC, and careful patient selection for MCS are important for optimal patient care.
脓毒症常导致血管麻痹和高动力心脏状态,治疗重点是恢复血管张力。然而,脓毒症也可引起可逆性心肌功能障碍,尤其是在患有基础心脏疾病的老年人中。《拯救脓毒症运动指南》建议,对于伴有心功能不全且在充分液体复苏和血压稳定的情况下仍持续存在低灌注的感染性休克患者,可单独使用多巴酚丁胺联合去甲肾上腺素或肾上腺素。然而,这些指南中心脏功能不全和低灌注的定义仍存在争议,导致临床解释各异。尽管恢复了足够的前负荷和后负荷,但仍存在持续低灌注的心脏功能不全通常被视为心源性休克。因此,脓毒症并发新发心肌功能障碍或因脓毒症诱导的心肌病导致基础心肌功能恶化,进而引发心源性休克,可定义为“脓毒症诱导的心源性休克(SICS)”。已知SICS与显著更高的死亡率相关。心脏功能障碍病史是SICS的有力预测指标,鉴于人口老龄化和心血管疾病患病率上升,凸显了精确诊断和管理的必要性。因此,与单纯感染性休克患者不同,SICS可能受益于使用肺动脉导管(PAC)进行早期有创血流动力学监测。虽然对所有脓毒症患者进行常规PAC监测不切实际,但超声心动图可能是高危个体的有用筛查工具。如果超声心动图提示心源性休克,则可能需要进行PAC持续监测。正性肌力药物在SICS中的作用仍不确定。对于重症病例,可考虑使用机械循环支持(MCS),因为高剂量血管加压药和正性肌力药物与更差的预后相关。正确选择患者是改善MCS治疗效果的关键。组建心源性休克治疗团队采取多学科方法可能有益。总之,解决SICS诊断和管理中的证据空白至关重要。超声心动图用于筛查、PAC进行高级监测以及仔细选择MCS患者对于优化患者护理很重要。