Holtan Shernan G, Bolaños-Meade Javier, Al Malki Monzr M, Wu Juan, Kitko Carrie L, Reshef Ran, Rezvani Andrew R, Shaffer Brian C, Solh Melhem M, Yao Janny M, Runaas Lyndsey, Elmariah Hany, Larkin Karilyn T, El Jurdi Najla, Gooptu Mahasweta, Loren Alison W, Hall Aric C, Alousi Amin M, Jamy Omer, Clark William, Kean Leslie, Bhatt Ami S, Perales Miguel-Angel, Applegate Kristy, Efebera Yvonne Adeduni, Leifer Eric, Jones Richard J, Horowitz Mary M, Mattila Deborah, Saber Wael, Hamadani Mehdi, Martens Michael J
Department of Medicine, Transplant and Cellular Therapy Program, Roswell Park Comprehensive Cancer Center, Buffalo, NY.
Bone Marrow Transplantation, The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Baltimore, MD.
J Clin Oncol. 2025 Mar 10;43(8):912-918. doi: 10.1200/JCO.24.00921. Epub 2025 Jan 3.
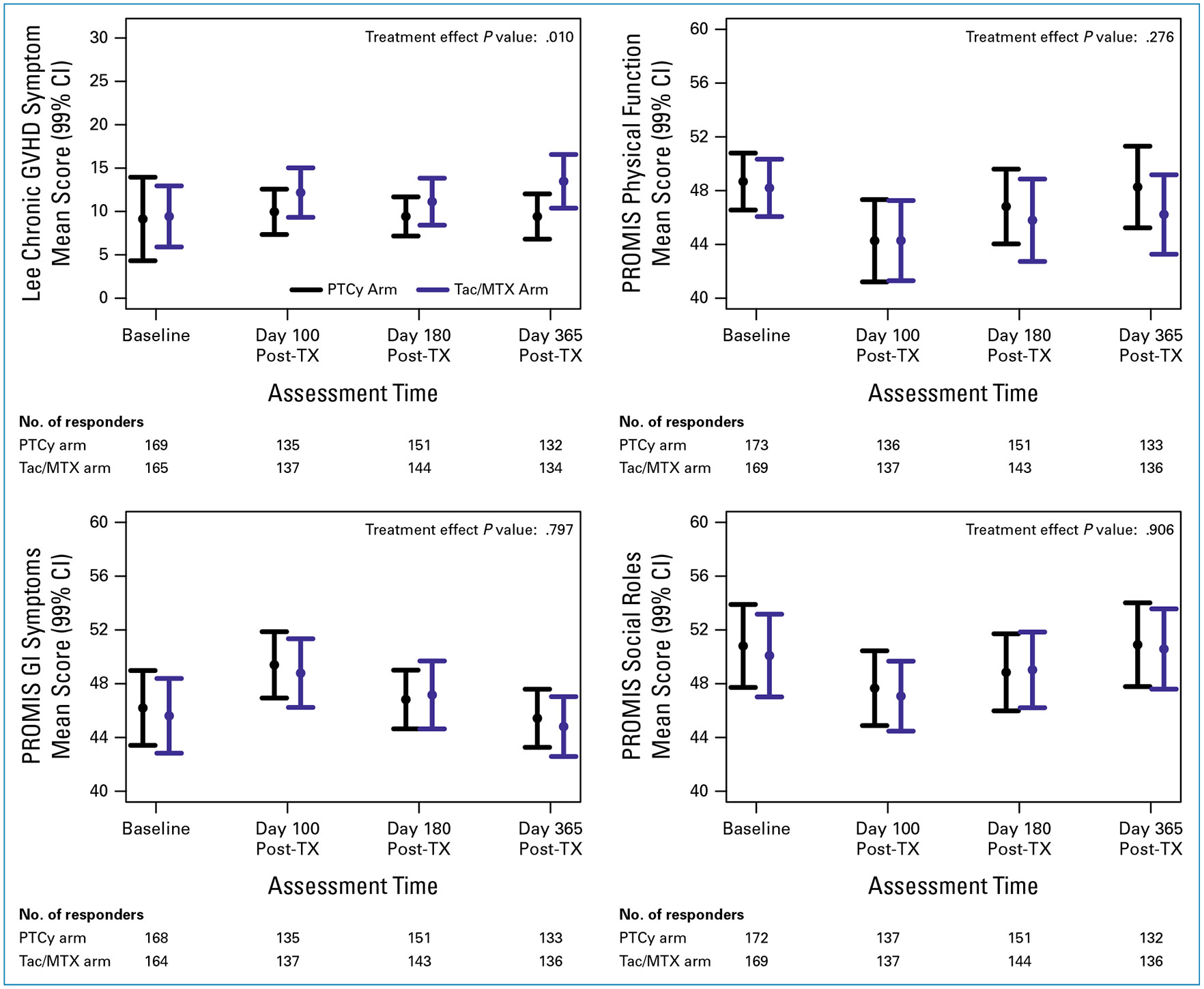
The BMT CTN 1703 phase III trial confirmed that graft-versus-host disease (GVHD) prophylaxis with post-transplantation cyclophosphamide (PTCy), tacrolimus (Tac), and mycophenolate mofetil (MMF) results in superior GVHD-free, relapse-free survival (GRFS) compared with Tac/methotrexate (MTX) prophylaxis. This companion study assesses the effect of these regimens on patient-reported outcomes (PROs). Using the Lee Chronic GVHD Symptom Score and PROMIS subscales (physical function, GI symptoms, social role satisfaction) as primary end points and hemorrhagic cystitis symptoms and Lee subscales as secondary end points, responses from English and Spanish speakers were analyzed at baseline and days 100, 180, and 365 after transplant. PRO scores were compared between the arms using inverse probability weighted-independent estimating equation models. The PTCy arm had significantly lower scores on the Lee Chronic GVHD Symptom Scale ( = .01), indicating lower GVHD symptom burden. Lee Scale nutrition and mouth subscores were also better in the PTCy arm compared with the Tac/MTX arm ( < .01 for both). Older participants (age >65 years) reported better Lee Scale psychological subscores than younger participants ( = .003). No significant differences were identified in hemorrhagic cystitis or in the PROMIS subscales between treatment arms. The updated clinical end points at 2 years for the parent trial confirmed that PTCy/Tac/MMF maintained a significant advantage over Tac/MTX in GRFS (42.4% 28.8%, = .001). In addition to improved GRFS, patients randomly assigned to the PTCy arm reported lower symptom burden during the first year after transplant.
BMT CTN 1703三期试验证实,与使用他克莫司(Tac)/甲氨蝶呤(MTX)进行移植物抗宿主病(GVHD)预防相比,采用移植后环磷酰胺(PTCy)、他克莫司(Tac)和霉酚酸酯(MMF)进行GVHD预防可带来更优的无GVHD、无复发生存期(GRFS)。这项配套研究评估了这些方案对患者报告结局(PROs)的影响。以Lee慢性GVHD症状评分和PROMIS子量表(身体功能、胃肠道症状、社会角色满意度)作为主要终点,以出血性膀胱炎症状和Lee子量表作为次要终点,对英语和西班牙语使用者在基线以及移植后第100天、180天和365天的反应进行了分析。使用逆概率加权独立估计方程模型对各治疗组之间的PRO评分进行比较。PTCy组在Lee慢性GVHD症状量表上的得分显著更低(P = 0.01),表明GVHD症状负担更低。与Tac/MTX组相比,PTCy组在Lee量表的营养和口腔子评分方面也更好(两者均P < 0.01)。老年参与者(年龄>65岁)报告的Lee量表心理子评分优于年轻参与者(P = 0.003)。在治疗组之间,出血性膀胱炎或PROMIS子量表方面未发现显著差异。母试验2年时的更新临床终点证实,PTCy/Tac/MMF在GRFS方面相对于Tac/MTX仍保持显著优势(42.4%对28.8%,P = 0.001)。除了GRFS得到改善外,随机分配到PTCy组的患者在移植后第一年报告的症状负担更低。