Sæter Mali, Johansen Sara Hassing, Reinertsen Kristin Valborg, Thorsen Lene, Haugaa Kristina Hermann, Nilsen Tormod Skogstad, Sarvari Sebastian Imre
Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway.
ProCardio Center for Innovation, Department of Cardiology, Oslo University Hospital, Oslo, Norway.
Cardiooncology. 2025 Jan 4;11(1):1. doi: 10.1186/s40959-024-00296-0.
Although anthracycline-related cardiotoxicity is widely studied, only a limited number of echocardiographic studies have assessed cardiac function in breast cancer survivors (BCSs) beyond ten years from anthracycline treatment, and the knowledge of long-term cardiorespiratory fitness (CRF) in this population is scarce. This study aimed to compare CRF assessed as peak oxygen uptake (V̇O), cardiac morphology and function, and cardiovascular (CV) risk factors between long-term BCSs treated with anthracyclines and controls with no history of cancer.
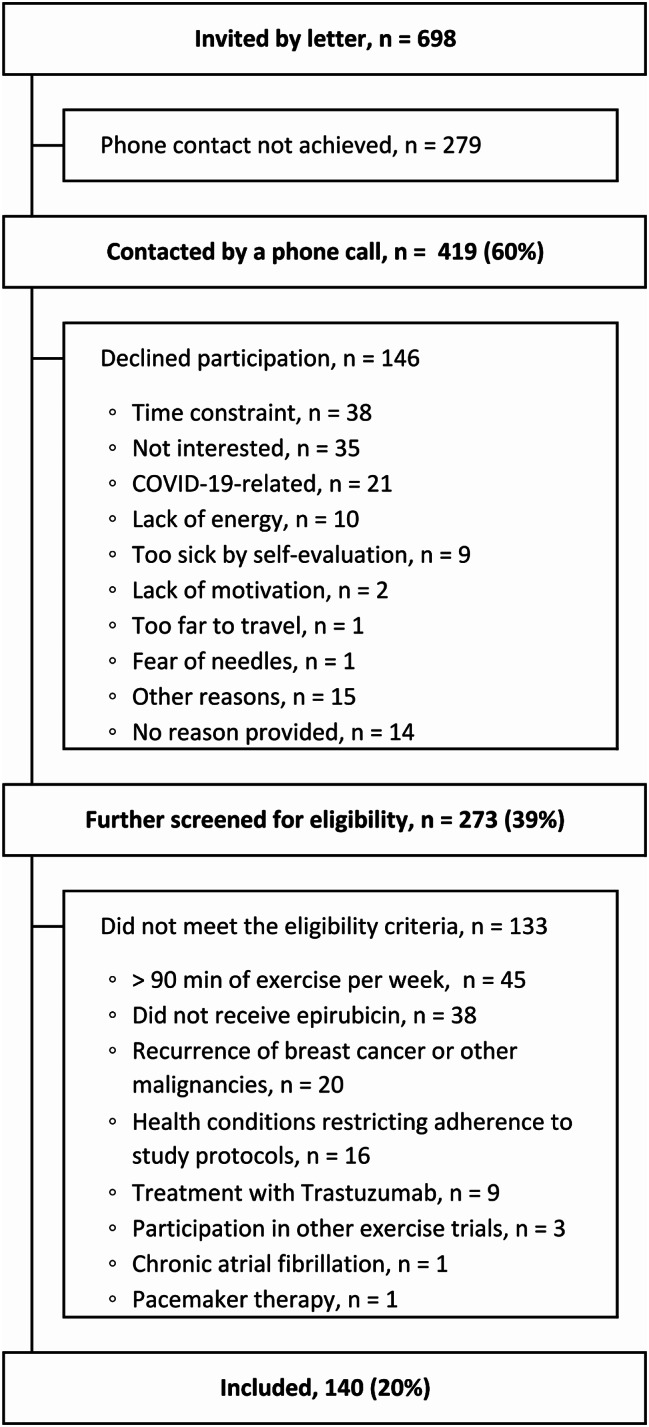
The CAUSE (Cardiovascular Survivors Exercise) trial included 140 BCSs recruited through the Cancer Registry of Norway, who were diagnosed with breast cancer stage II to III between 2008 and 2012 and had received treatment with epirubicin, and 69 similarly aged activity level-matched controls. All the participants underwent blood sampling, blood pressure measurements, echocardiography and cardiopulmonary exercise testing from October 2020 to August 2022.
BCSs were aged 59 ± 6 years and had received a cumulative dose of 357 (243 to 366) mg/m of epirubicin on average 11 ± 1 years before inclusion. There was no difference between BCSs and controls with respect to peak V̇O (27.6 ± 5.4 mL/kg/min vs. 27.1 ± 5.4 mL/kg/min, P = 0.25), 2D left ventricular ejection fraction (57 ± 3% vs. 57 ± 3%, P = 0.43), left ventricular global longitudinal strain (-20.5 ± 1.0% vs. -20.6 ± 1.0%, P = 0.46) or the proportion with N-terminal pro-brain natriuretic peptide ≥ 125 (22% vs. 20%, P = 0.93). The proportions with hypertension, dyslipidemia or diabetes did not differ between the groups.
We found that CRF, cardiac function, and CV risk profile in BCSs examined a decade after treatment with anthracyclines were similar to that in women with no history of cancer.
clinicaltrials.gov (NCT04307407) https://clinicaltrials.gov/ct2/show/NCT04307407 .
尽管蒽环类药物相关的心脏毒性已得到广泛研究,但仅有少数超声心动图研究评估了蒽环类药物治疗十年后的乳腺癌幸存者(BCS)的心脏功能,且该人群长期心肺适能(CRF)的相关知识匮乏。本研究旨在比较接受蒽环类药物治疗的长期BCS与无癌症病史的对照组之间,以峰值摄氧量(V̇O)评估的CRF、心脏形态和功能以及心血管(CV)危险因素。
CAUSE(心血管幸存者运动)试验纳入了140名通过挪威癌症登记处招募的BCS,他们在2008年至2012年期间被诊断为II至III期乳腺癌,并接受了表柔比星治疗,以及69名年龄相仿、活动水平匹配的对照组。所有参与者在2020年10月至2022年8月期间接受了血液采样、血压测量、超声心动图检查和心肺运动测试。
BCS的年龄为59±6岁,在纳入研究前平均11±1年接受了累积剂量为357(243至366)mg/m²的表柔比星治疗。BCS与对照组在峰值V̇O(27.6±5.4 mL/kg/min对27.1±5.4 mL/kg/min,P = 0.25)、二维左心室射血分数(57±3%对57±3%,P = 0.43)、左心室整体纵向应变(-20.5±1.0%对-20.6±1.0%,P = 0.46)或N末端脑钠肽前体≥125的比例(22%对20%,P = 0.93)方面无差异。两组间高血压、血脂异常或糖尿病的比例也无差异。
我们发现,蒽环类药物治疗十年后接受检查的BCS的CRF、心脏功能和CV风险状况与无癌症病史的女性相似。
clinicaltrials.gov(NCT04307407)https://clinicaltrials.gov/ct2/show/NCT04307407 。