Kitson-Mills Doris, Donkor Andrew, Amoako Yaw Ampem, Kyei Kofi Adesi, Bonsu Ernest Barwuah Osei, Vanderpuye Verna, Wiafe Yaw Amo
Department of Medical Imaging, Faculty of Allied Health Sciences, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana.
Improving Palliative, Aged and Chronic Care through Clinical Research and Translation (IMPACCT), Faculty of Health, University of Technology Sydney, Sydney, New South Wales, Australia.
Adv Radiat Oncol. 2024 Nov 6;10(1):101670. doi: 10.1016/j.adro.2024.101670. eCollection 2025 Jan.
Current management for clinically localized prostate cancer in low- and middle-income countries (LMICs) includes surgery, external beam radiation therapy (EBRT), and brachytherapy either alone or in combination, with plus or minus hormone therapy. The toxicity profiles and oncological outcomes of these treatment modalities vary. This systematic review and meta-analysis aimed to determine the prevalence of treatment-related outcomes and toxicities for men diagnosed with localized prostate cancer in LMICs.
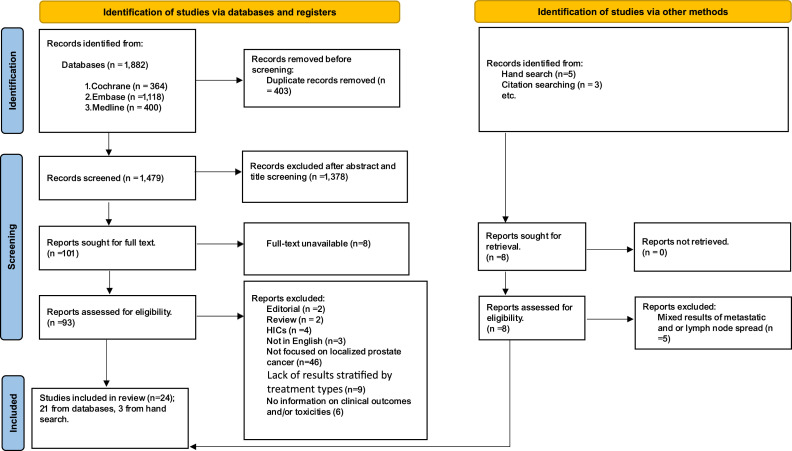
The review was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Cochrane Library, Embase, and Medline were searched for eligible articles. Meta-analysis was performed with Review Manager version 5.4.1 using a random effects model at a 95% confidence interval.
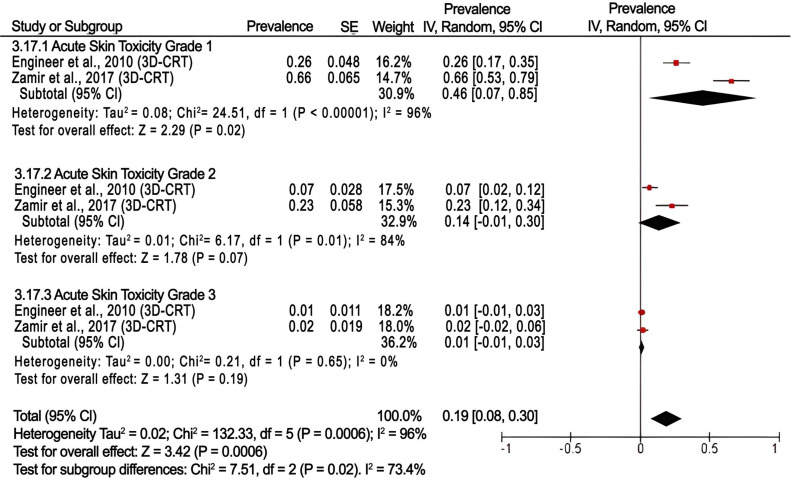
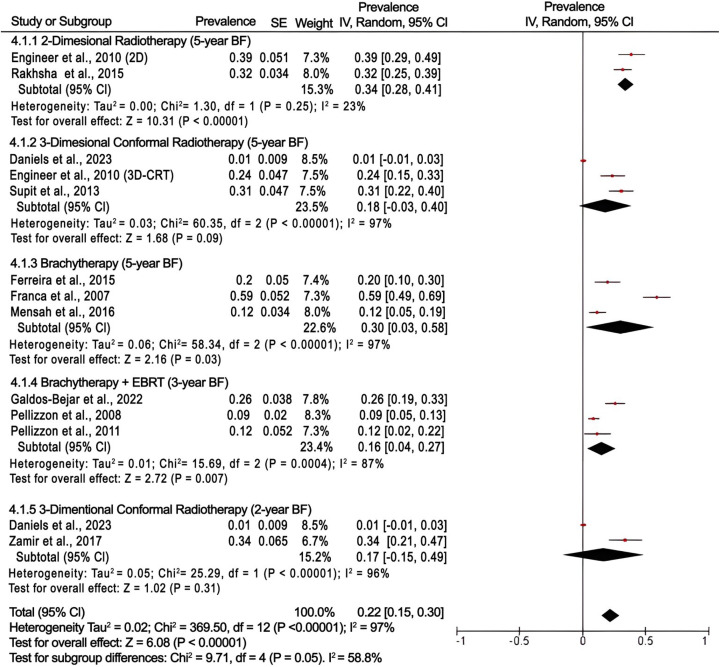
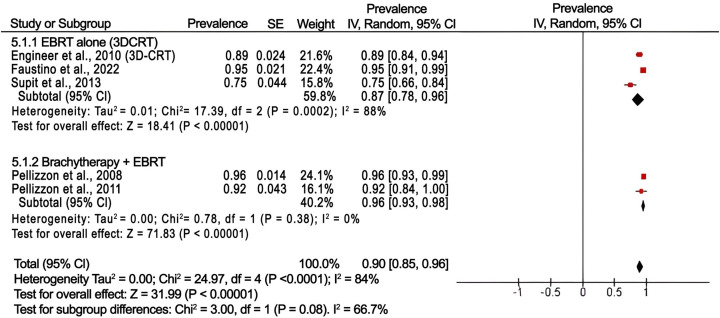
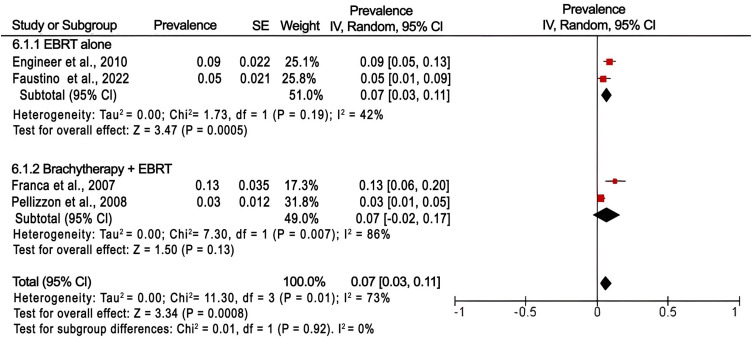
A total of 2,820 patients were analyzed from 24 articles that met the inclusion criteria. Following 3-dimensional conformal radiation therapy (3D-CRT), the most common clinician-reported toxicities were acute skin grade 1, acute genitourinary grade 1, acute gastrointestinal grade 1, and late gastrointestinal grade 1, with 46%, 29%, 24%, and 18%, respectively. Acute and late genitourinary grade 3 and gastrointestinal grade 3 toxicities were below 3% with no grade 4 toxicities reported after 3D-CRT. In the brachytherapy group, the prevalence of acute genitourinary grade 1 toxicity was 19%. Perioperative rectal injury was the least prevalent (2%) after retropubic radical prostatectomy. Following 3D-CRT, the 5-year overall survival rate was 87%, and for the combined brachytherapy and EBRT group, it increased to 96%. The prevalence of 5-year biochemical failure following EBRT and brachytherapy was 18% and 30%, respectively. The 4- and 3-year biochemical failure after radical prostatectomy and combined EBRT with brachytherapy were 22% and 2%, respectively.
This systematic review and meta-analysis indicate that in LMICs, EBRT, brachytherapy, and radical prostatectomy, either alone or in combination has an excellent potential for localized prostate cancer control with low toxicities and good oncological outcomes. Results of treatment-related toxicities and outcomes can support policymakers, patients, and clinicians on informed decision-making to strengthen prostate cancer care in the region. However, efforts are required to improve early detection, treatment accessibility, regular post-treatment follow-up care, consistent quality assurance practices, and staff continues development to help minimize treatment toxicities and improve outcomes of localized prostate cancer in LMICs.
低收入和中等收入国家(LMICs)中临床局限性前列腺癌的当前治疗方法包括手术、外照射放疗(EBRT)和近距离放疗,可单独使用或联合使用,加或不加激素治疗。这些治疗方式的毒性特征和肿瘤学结果各不相同。本系统评价和荟萃分析旨在确定LMICs中被诊断为局限性前列腺癌的男性患者与治疗相关的结果和毒性的发生率。
本评价依据系统评价和荟萃分析的首选报告项目指南进行。在Cochrane图书馆、Embase和Medline中检索符合条件的文章。使用Review Manager 5.4.1版本,采用随机效应模型在95%置信区间进行荟萃分析。
从24篇符合纳入标准的文章中总共分析了2820例患者。在三维适形放疗(3D-CRT)后,临床医生报告的最常见毒性为急性皮肤1级、急性泌尿生殖系统1级、急性胃肠道1级和晚期胃肠道1级,发生率分别为46%、29%、24%和18%。急性和晚期泌尿生殖系统3级和胃肠道3级毒性低于3%,3D-CRT后未报告4级毒性。在近距离放疗组中,急性泌尿生殖系统1级毒性的发生率为19%。耻骨后根治性前列腺切除术后围手术期直肠损伤发生率最低(2%)。3D-CRT后,5年总生存率为87%,对于近距离放疗和EBRT联合组,该生存率提高到96%。EBRT和近距离放疗后5年生化失败的发生率分别为18%和30%。根治性前列腺切除术后以及EBRT与近距离放疗联合后的4年和3年生化失败率分别为22%和2%。
本系统评价和荟萃分析表明,在LMICs中,EBRT、近距离放疗和根治性前列腺切除术,单独或联合使用,在控制局限性前列腺癌方面具有巨大潜力,毒性低且肿瘤学结果良好。治疗相关毒性和结果的研究结果可为政策制定者、患者和临床医生提供信息,以支持他们做出明智决策,加强该地区的前列腺癌护理。然而,需要努力改善早期检测、治疗可及性、定期的治疗后随访护理、一致的质量保证措施以及工作人员的持续发展,以帮助将LMICs中局限性前列腺癌的治疗毒性降至最低并改善治疗结果。