Rostami Mohsen, Varela Jesus Roberto, Kerolus Mena G, DeWald Christopher J, Fontes Ricardo B V
Department of Neurosurgery, Rush University Medical Center, Chicago, Illinois.
Atlanta Brain and Spine Care, Atlanta, Georgia.
J Neurosurg Case Lessons. 2025 Jan 6;9(1). doi: 10.3171/CASE24664.
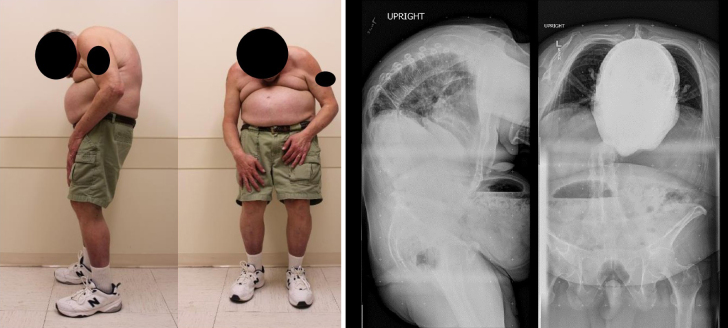
Kyphotic spinal deformity is a complication of ankylosing spondylitis (AS). In rare cases, particularly in obese patients, the deformity might extend to the cervicothoracic spine, resulting in a severe "chin-on-abdomen" deformity. This condition severely impairs quality of life by affecting gaze, swallowing, and causing chronic pain. While corrective surgery is often performed for lumbar and thoracic kyphosis, cases involving global kyphotic deformities are less common.
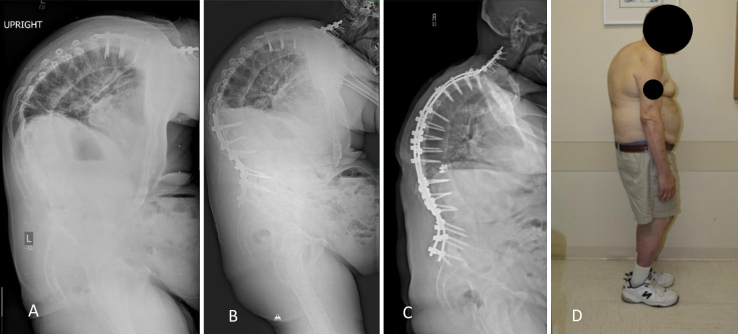
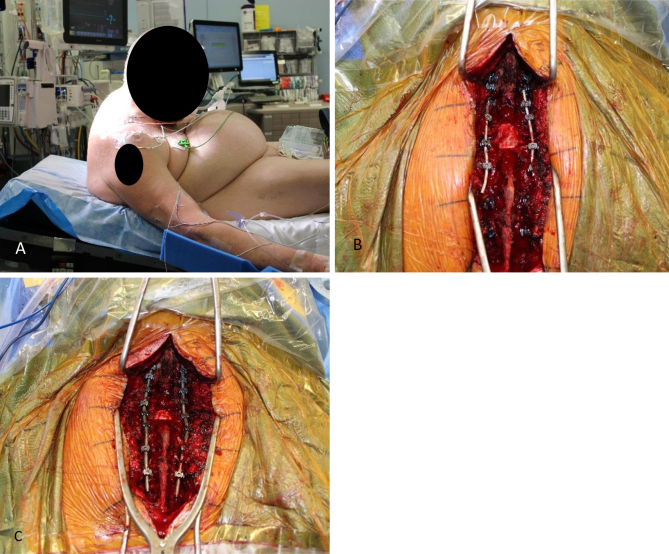
The authors present the case of a 66-year-old obese man with AS and a chin-on-abdomen deformity. Prone positioning for surgery was not feasible due to his body habitus. A three-stage corrective surgery was performed: a C7 extension osteotomy in a semisitting position, an L3 pedicle subtraction osteotomy in the lateral decubitus position, and a T11 vertebral column resection in the prone position. The first stage utilized a seldom-used, earlier osteotomy technique with modern instrumentation and neuromonitoring. Obesity again precluded prone positioning in the second stage, necessitating surgery in the lateral position. Postoperatively, the patient exhibited significant postural improvement, maintained over a 5-year follow-up period.
This case underscores the importance of adaptable techniques and positioning strategies in correcting complex spinal deformities in obese patients with AS. Integrating traditional methods with modern technology is crucial for achieving successful outcomes. https://thejns.org/doi/10.3171/CASE24664.
脊柱后凸畸形是强直性脊柱炎(AS)的一种并发症。在罕见情况下,尤其是肥胖患者,畸形可能会延伸至颈胸段脊柱,导致严重的“下巴贴腹”畸形。这种情况会影响视力、吞咽并引发慢性疼痛,严重损害生活质量。虽然通常对腰椎和胸椎后凸进行矫正手术,但涉及整体后凸畸形的病例较少见。
作者报告了一例66岁患有AS且有下巴贴腹畸形的肥胖男性病例。由于其身体状况,手术俯卧位不可行。进行了三阶段矫正手术:在半坐位进行C7延长截骨术,在侧卧位进行L3椎弓根截骨术,在俯卧位进行T11椎体切除术。第一阶段采用了一种较少使用的早期截骨技术,并结合了现代器械和神经监测。肥胖再次使第二阶段无法采用俯卧位,因此必须在侧卧位进行手术。术后,患者的姿势有显著改善,在5年随访期内保持良好。
该病例强调了在矫正AS肥胖患者复杂脊柱畸形时,采用适应性技术和体位策略的重要性。将传统方法与现代技术相结合对于取得成功结果至关重要。https://thejns.org/doi/10.3171/CASE24664 。