Enciu Octavian, Toma Elena-Adelina, Miron Adrian, Popa Gabriela Loredana, Muntean Andrei-Alexandru, Porosnicu Andrei Ludovic, Popa Mircea Ioan
Department of Microbiology, "Cantacuzino" Institute, "Carol Davila" University of Medicine and Pharmacy, 020021 Bucharest, Romania.
Emergency Hospital-Surgery Department, Elias University, 020021 Bucharest, Romania.
Antibiotics (Basel). 2024 Dec 1;13(12):1150. doi: 10.3390/antibiotics13121150.
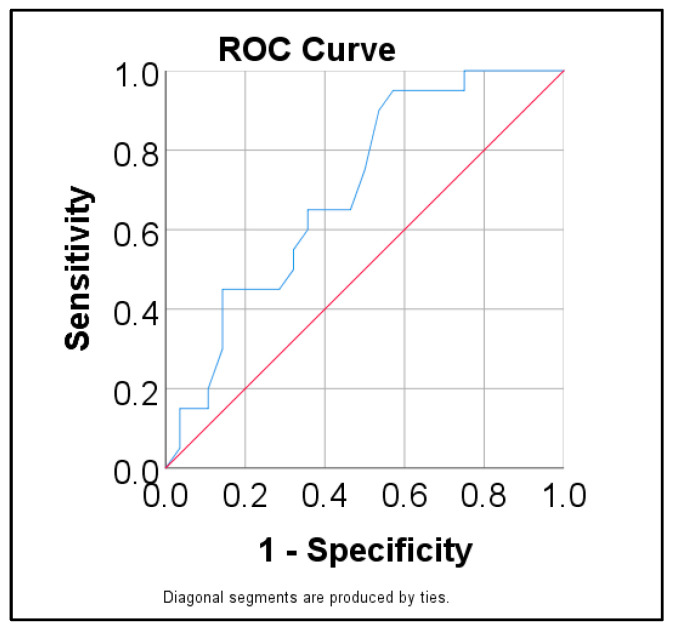
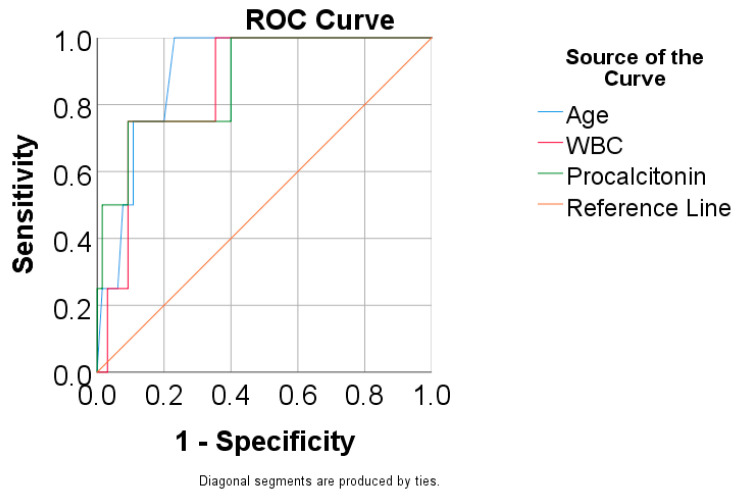
Antimicrobial resistance is one of the main threats to public health, with multidrug-resistant (MDR) pathogens on the rise across continents. Although treatment guidelines generally recommend antimicrobial therapy for acute complicated diverticulitis, they do not specify treatment pathways according to local or national resistance profiles. There is sparse data regarding specific pathogens involved in Hinchey II-IV patients who undergo surgery. This study seeks to address these issues and determine how often and what types of MDR bacteria occur in patients undergoing emergency surgery. We prospectively enrolled patients admitted between 2020-2023 and who underwent emergency surgery for complicated acute diverticulitis. We analysed the inflammatory response parameters at admission, the type of surgery employed for source control, identified pathogens in the peritoneal samples, their antimicrobial susceptibility, the efficacy of antimicrobial empiric therapy, and mortality. Gram-negative bacteria were identified most often, with being mostly MDR (43.9%) or extended-spectrum beta-lactamase producing (ESBL +ve) (24.4%), while most strains of were extended-spectrum beta-lactamase positive (ESBL +ve) (80%) and MDR (80%). Of the spp., 57.14% were vancomycin-resistant (VRE) strains. Patients with Hinchey III/IV were significantly more associated with MDR. Patients with multiple pathogens were significantly associated with ESBL+/VRE strains. Age, leucocytosis, and procalcitonin levels at admission were good indicators for mortality prediction, which occurred in four cases. In an age when antibiotic stewardship is advisable especially in emergency settings, the treatment should be tailored according to local profiles of MDR to ensure adequate outcomes for patients.
抗菌药物耐药性是对公众健康的主要威胁之一,多重耐药(MDR)病原体在各大洲呈上升趋势。尽管治疗指南通常推荐对急性复杂性憩室炎进行抗菌治疗,但并未根据当地或国家的耐药情况指定治疗途径。关于接受手术的欣奇(Hinchey)II-IV级患者中涉及的特定病原体的数据很少。本研究旨在解决这些问题,并确定急诊手术患者中MDR细菌出现的频率和类型。我们前瞻性地纳入了2020年至2023年间入院并因复杂性急性憩室炎接受急诊手术的患者。我们分析了入院时的炎症反应参数、用于源头控制的手术类型、腹膜样本中鉴定出的病原体、它们的抗菌药敏性、抗菌经验性治疗的疗效以及死亡率。革兰氏阴性菌最常被鉴定出来,其中大多是MDR(43.9%)或产超广谱β-内酰胺酶(ESBL+)(24.4%),而大多数菌株是超广谱β-内酰胺酶阳性(ESBL+)(80%)和MDR(80%)。在肠球菌属中,57.14%是耐万古霉素(VRE)菌株。欣奇III/IV级患者与MDR的相关性显著更高。有多种病原体的患者与ESBL+/VRE菌株的相关性显著。入院时的年龄、白细胞增多和降钙素原水平是死亡率预测的良好指标,有4例患者死亡。在一个尤其在急诊环境中提倡抗生素管理的时代,治疗应根据当地的MDR情况进行调整,以确保患者获得足够的治疗效果。