Rosas-Díaz José, Guerrero Maria Eugenia, Córdova-Limaylla Nancy, Galindo-Gómez Maisely, García-Luna Marco, Cayo-Rojas César
School of Stomatology, Universidad Privada San Juan Bautista, Lima 15067, Peru.
Faculty of Stomatology, Universidad Peruana Cayetano Heredia, Lima 15102, Peru.
Biomedicines. 2024 Dec 18;12(12):2878. doi: 10.3390/biomedicines12122878.
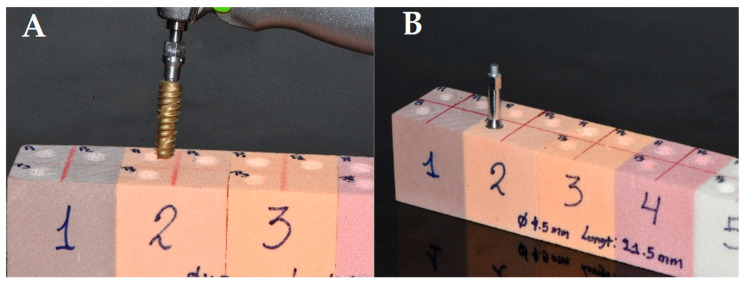
: This study aimed to evaluate the primary stability, according to the insertion torque value (ITV) and resonance frequency analysis (RFA), of dental implants placed in standardized blocks of bone quality equivalent to type II-A bone, using three surgical undersized protocols of 0.2 mm, 0.5 mm, and 0.8 mm, considering different dental implant diameters and lengths. : One hundred and twenty dental implants (DIs) of different diameters (3.5, 3.8, 4.5, and 5.0 mm) and lengths (8.5, 10.0, 11.5, 13.0, and 15.0 mm) placed in polyurethane blocks equivalent to type II-A bone, according to the Lekholm and Zarb classification modified by Rosas et al., were examined with three surgical protocols of under-milling of 0.2, 0.5, and 0.8 mm. The ITV and the RFA were the determinants of primary stability, and their respective values were recorded as Ncm and the implant stability quotient (ISQ) immediately after the placement of the DIs. These were evaluated according to each surgical insertion protocol, length, and diameter of the DI under a multivariate analysis model (MANOVA). Statistical significance was set at < 0.05. : It was observed that the average of the ITV was significantly higher when a 0.8 mm under-milling protocol was used (63.2 ± 14.9 Ncm) ( < 0.001). However, the ITV was significantly lower when a 0.2 mm under-milling protocol was used (25.1 ± 8.3 Ncm) ( < 0.001). On the other hand, the ISQ did not present significant differences ( = 0.166) when comparing the 0.2 (67.6 ISQ ± 5.4 ISQ), 0.5 (65.8 ISQ ± 3.4 ISQ), and 0.8 (65.7 ISQ ± 4.0 ISQ) under-milling protocols in the evaluation of the primary stability of the dental implant. The multivariate effect size (η = 0.639) indicated that the variability detected in the insertion torque and the ISQ, at the same time, was explained by 63.9% ( < 0.001) due only to the compression protocol, while the implant diameter explained this variability by 27.0% (η = 0.270) ( < 0.001) and the implant length only significantly explained this variability by 12.1% (η = 0.121) ( = 0.030). Finally, any interaction between the compression protocol, implant diameter, and length did not influence insertion torque variability or the ISQ ( > 0.05). : It can be concluded that when the surgical protocol for subpreparation is optimal according to the prepared bone bed, regardless of the diameter or length of the dental implant used, primary stability was assured according to the ITV and the RFA in 63.9%. This finding allows us to recommend carrying out a correct analysis of bone quality in order to subsequently select the most appropriate surgical protocol for the subpreparation of the bone bed to achieve better primary stability of the dental implant.
本研究旨在根据植入扭矩值(ITV)和共振频率分析(RFA),评估使用0.2毫米、0.5毫米和0.8毫米三种手术预备不足方案,将牙种植体植入等同于II - A型骨质量的标准化骨块中时的初期稳定性,同时考虑不同的牙种植体直径和长度。
根据Rosas等人修改的Lekholm和Zarb分类法,将120颗不同直径(3.5毫米、3.8毫米、4.5毫米和5.0毫米)和长度(8.5毫米、10.0毫米、11.5毫米、13.0毫米和15.0毫米)的牙种植体植入等同于II - A型骨的聚氨酯块中,并采用0.2毫米、0.5毫米和0.8毫米的三种手术预备不足方案进行检查。ITV和RFA是初期稳定性的决定因素,在牙种植体植入后立即将它们各自的值记录为牛顿厘米(Ncm)和种植体稳定性商数(ISQ)。在多变量分析模型(MANOVA)下,根据每种手术植入方案、牙种植体的长度和直径对这些数据进行评估。统计学显著性设定为<0.05。
观察到,使用0.8毫米预备不足方案时,ITV的平均值显著更高(63.2±14.9 Ncm)(<0.001)。然而,使用0.2毫米预备不足方案时,ITV显著更低(25.1±8.3 Ncm)(<0.001)。另一方面,在评估牙种植体的初期稳定性时,比较0.2(67.6 ISQ±5.4 ISQ)、0.5(65.8 ISQ±3.4 ISQ)和0.8(65.7 ISQ±4.0 ISQ)毫米预备不足方案时,ISQ没有呈现显著差异(=0.166)。多变量效应大小(η = 0.639)表明,仅由于压缩方案,在植入扭矩和ISQ中同时检测到的变异性有63.9%(<0.001)得到了解释,而种植体直径对这种变异性的解释为27.0%(η = 0.270)(<0.001),种植体长度仅对这种变异性有显著解释力,为12.1%(η = 0.121)(=0.030)。最后,压缩方案、种植体直径和长度之间的任何相互作用均未影响植入扭矩变异性或ISQ(>0.05)。
可以得出结论,当根据预备好的骨床使手术预备不足方案达到最佳时,无论所使用的牙种植体的直径或长度如何,根据ITV和RFA,63.9%的初期稳定性能够得到保证。这一发现使我们建议对骨质量进行正确分析,以便随后选择最合适的骨床手术预备不足方案,从而实现牙种植体更好的初期稳定性。