Ghosh Soma, O'Hara Madison P, Sinha Pragya, Mazumdar Tuhina, Yapindi Lacin, Sastry Jagannadha K, Johnson Faye M
Department of Thoracic, Head and Neck Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA.
The University of Texas at Austin College of Pharmacy, Austin, Texas, USA.
J Immunother Cancer. 2025 Jan 7;13(1):e009316. doi: 10.1136/jitc-2024-009316.
Human papillomavirus (HPV)-driven cancers include head and neck squamous cell carcinoma and cervical cancer and represent approximately 5% of all cancer cases worldwide. Standard-of-care chemotherapy, radiotherapy, and immune checkpoint inhibitors (ICIs) are associated with adverse effects and limited responses in patients with HPV-driven cancers. The integration of targeted therapies with ICIs may improve outcomes. In a previous study, we demonstrated that Aurora kinase A (, Aurora A) inhibitors lead to apoptosis of human HPV-positive cancer cells in vitro and in vivo. Here, we explored the potential of Aurora A inhibition to enhance response to ICIs in immune-competent preclinical models of HPV-driven cancers.
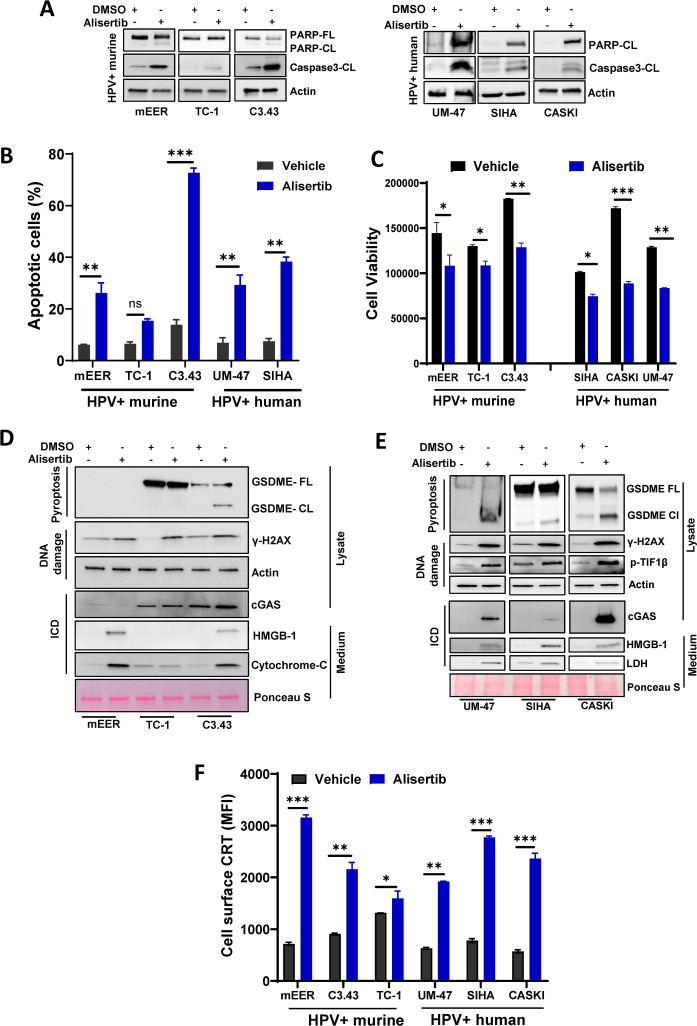
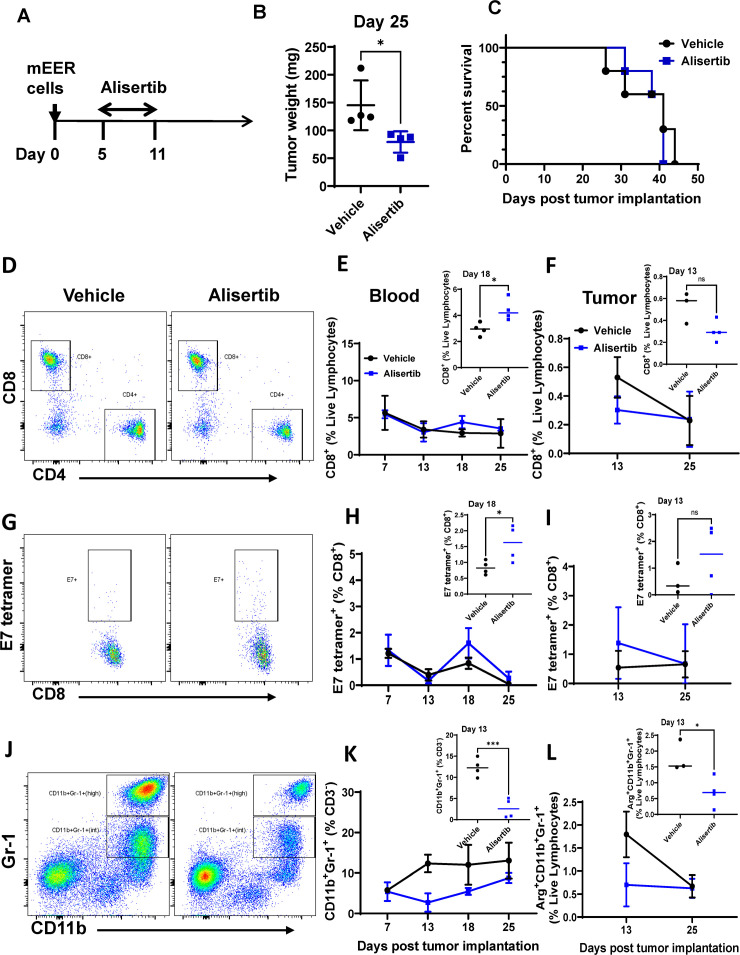
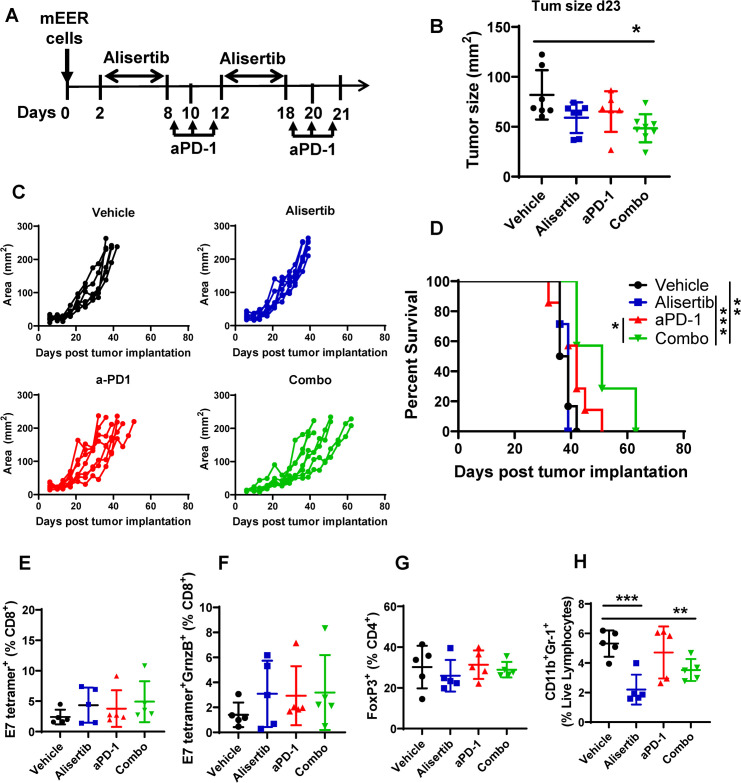
We assessed the induction of apoptosis, DNA damage, and immunogenic cell death (ICD) in response to treatment with the Aurora A inhibitor alisertib in vitro and antitumor efficacy of alisertib as a monotherapy and in combination with ICIs that inhibit programmed cell death protein-1 (PD-1) or cytotoxic T-lymphocyte associated protein 4 (CTLA-4) in murine HPV-positive immune-competent tumor models. In each treatment group, we determined the tumor growth kinetics and long-term survival and assessed the tumor immune microenvironment using polychromatic flow cytometry.
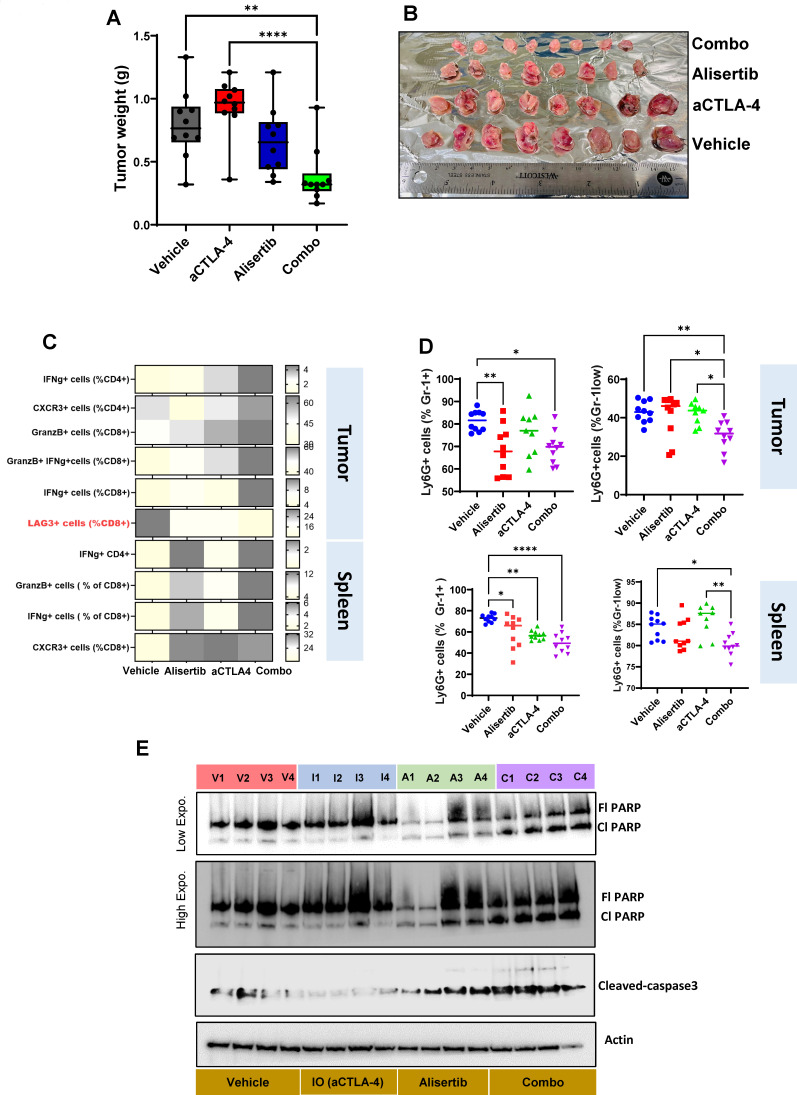
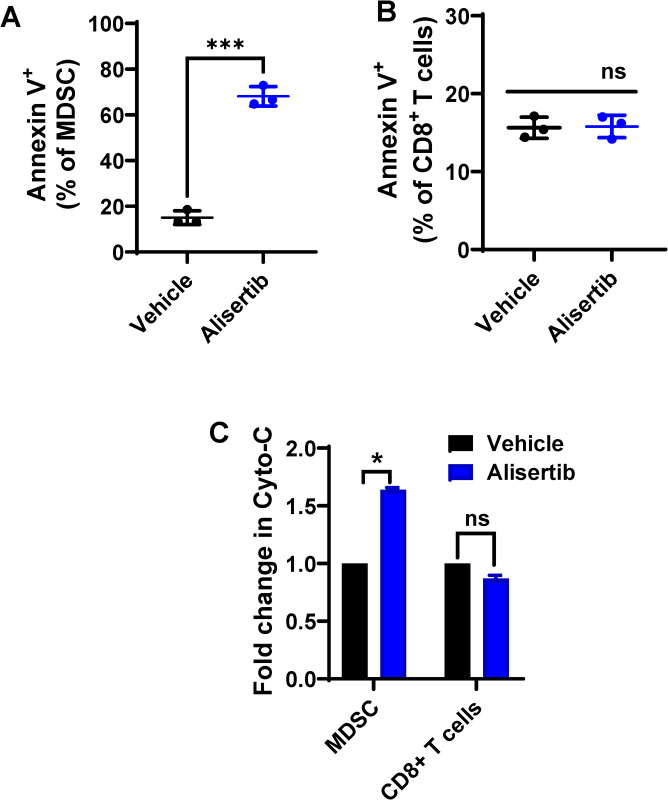
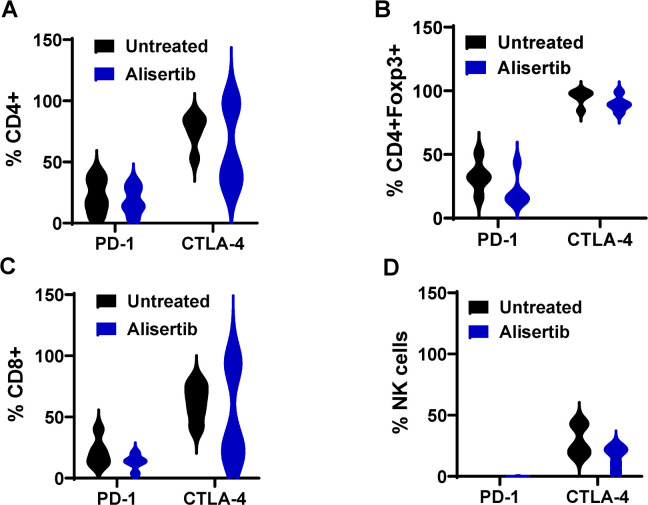
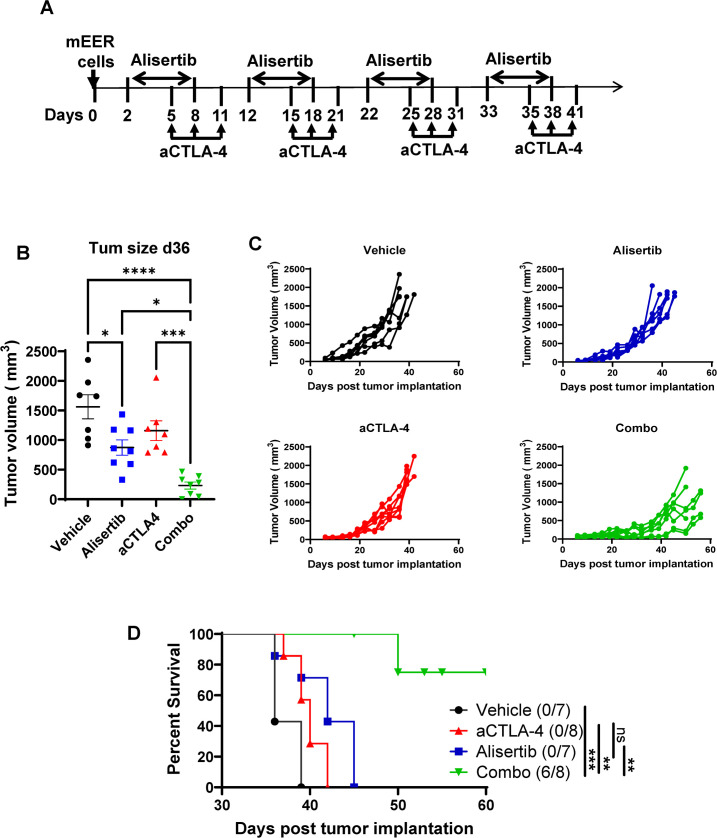
Aurora A inhibition induced apoptosis, DNA damage, and ICD in vitro in multiple human and murine HPV-positive cancer cell lines. Importantly, Aurora A inhibition induced selective apoptotic depletion of myeloid-derived suppressor cells (MDSCs). In vivo experiments demonstrated that the combination of alisertib with ICIs, specifically anti-CTLA4, resulted in improved survival outcomes by altering the tumor immune microenvironment. This combination enhanced CD8 T-cell infiltration and decreased the frequencies of MDSCs, whereas neither alisertib nor ICIs (anti-PD-1/anti-CTLA-4) alone showed such effects.
Our study establishes the potential of Aurora A inhibition to sensitize HPV-positive tumors to ICIs, specifically anti-CTLA-4 treatment. This combination strategy resulted in enhanced antitumor efficacy, driven by systemic and intratumoral increases in CD8 T-cell responses and reduced immunosuppressive cell populations, specifically MDSCs. These findings offer insights into the synergistic effects of Aurora A inhibition and ICIs and argue for further investigation and optimization of this combination approach in HPV-driven cancers.
人乳头瘤病毒(HPV)相关癌症包括头颈鳞状细胞癌和宫颈癌,约占全球所有癌症病例的5%。标准治疗的化疗、放疗和免疫检查点抑制剂(ICI)对HPV相关癌症患者有不良反应且疗效有限。靶向治疗与ICI联合使用可能改善治疗结果。在之前的一项研究中,我们证明极光激酶A(Aurora A)抑制剂在体外和体内均可导致人HPV阳性癌细胞凋亡。在此,我们在具有免疫活性的HPV相关癌症临床前模型中探索了抑制Aurora A增强对ICI反应的潜力。
我们评估了在体外使用Aurora A抑制剂阿利西替尼治疗后诱导的凋亡、DNA损伤和免疫原性细胞死亡(ICD),以及阿利西替尼作为单一疗法和与抑制程序性细胞死亡蛋白1(PD-1)或细胞毒性T淋巴细胞相关蛋白4(CTLA-4)的ICI联合使用时在小鼠HPV阳性免疫活性肿瘤模型中的抗肿瘤疗效。在每个治疗组中,我们确定肿瘤生长动力学和长期生存率,并使用多色流式细胞术评估肿瘤免疫微环境。
抑制Aurora A在体外可诱导多种人和小鼠HPV阳性癌细胞系发生凋亡、DNA损伤和ICD。重要的是,抑制Aurora A可诱导髓源性抑制细胞(MDSC)选择性凋亡性耗竭。体内实验表明,阿利西替尼与ICI联合使用,特别是与抗CTLA4联合使用,可通过改变肿瘤免疫微环境改善生存结果。这种联合增强了CD8 T细胞浸润,降低了MDSC频率,而单独使用阿利西替尼或ICI(抗PD-1/抗CTLA-4)均未显示出此类效果。
我们的研究证实了抑制Aurora A使HPV阳性肿瘤对ICI敏感,特别是对抗CTLA-4治疗敏感的潜力。这种联合策略通过全身和肿瘤内CD8 T细胞反应增加以及免疫抑制细胞群(特别是MDSC)减少,导致抗肿瘤疗效增强。这些发现为Aurora A抑制和ICI的协同作用提供了见解,并支持在HPV相关癌症中进一步研究和优化这种联合方法。