Schumacher Aurelian, Hieke Alina, Spenner Marie, Schmitz Fynn, Sgodzai Melissa, Klimas Rafael, Brünger Jil, Huckemann Sophie, Motte Jeremias, Fisse Anna Lena, Gold Ralf, Pitarokoili Kalliopi, Grüter Thomas
Department of Neurology, St. Josef Hospital, Ruhr University Bochum, 44791, Bochum, Germany.
Immune-Mediated Neuropathies Biobank (INHIBIT), Ruhr-University Bochum, Bochum, Germany.
J Neurol. 2025 Jan 7;272(1):100. doi: 10.1007/s00415-024-12860-w.
Diagnosing chronic inflammatory demyelinating polyneuropathy (CIDP) can be challenging, leading to delays in initiating therapy. As disability in CIDP is mainly dependent on axonal damage, the impact of delayed immunotherapy remains unclear. We multimodally investigated the clinical outcomes of patients with early CIDP regarding different treatment strategies and time points.
Patients with CIDP diagnosis within 1 year before study inclusion were systematically selected from the prospective Immune-mediated Neuropathies Biobank (INHIBIT) registry. Clinical and therapeutic data, and findings from nerve conduction study (NCS), and nerve and muscle ultrasound were correlated at inclusion and 12 months later. The patient outcomes were compared between immunotherapies. The effect of timing immunotherapy on clinical outcomes was determined using regression analysis.
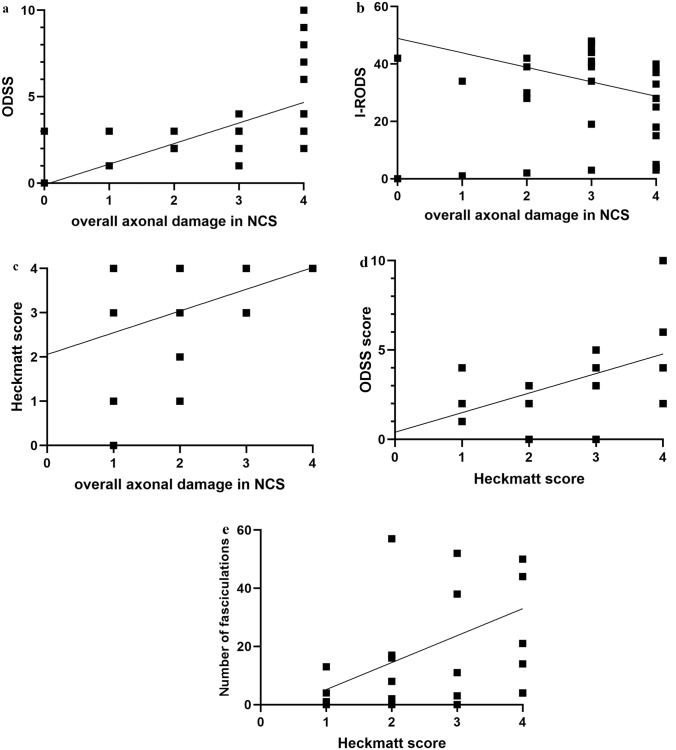
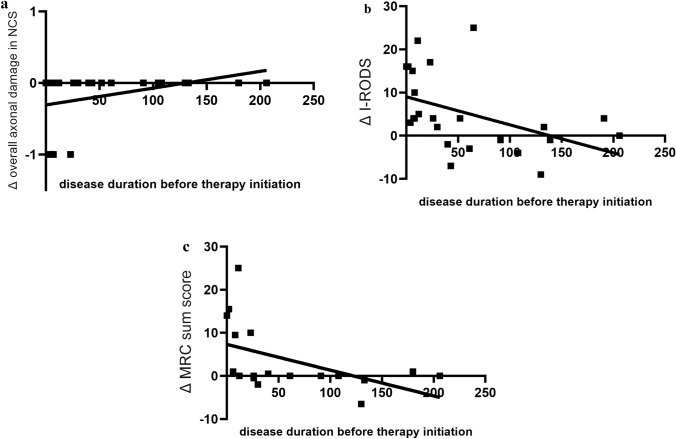
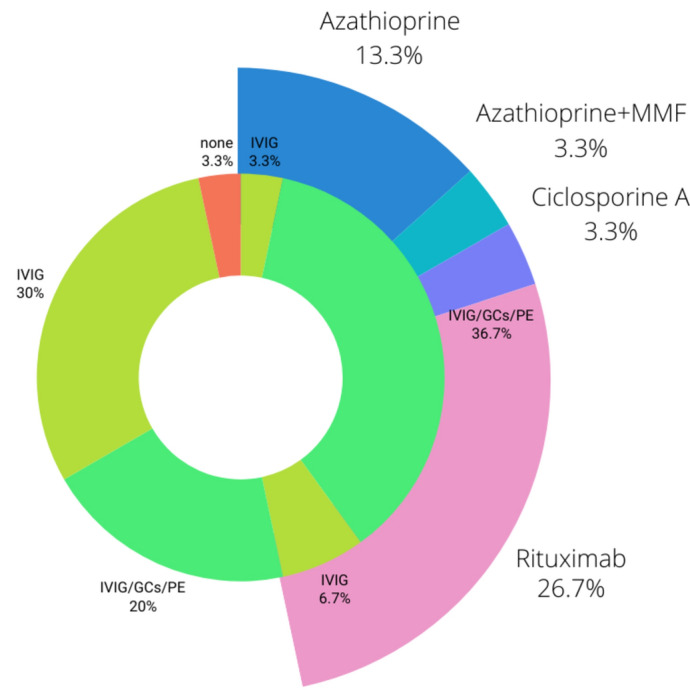
In total, 30 patients were included (time from diagnosis to inclusion 22 ± 19 weeks). Low amplitudes of compound muscle potential were significantly associated with pathological spontaneous activity (PSA, r = 0.467) and correlated with the Heckmatt scale (r = 0.391). All three parameters were significantly associated with higher overall disability sum scores (NCS score r = 0.581, PSA r = 0.385, Heckmatt scale r = 0.472). The delays in initiating therapy resulted in progression of axonal damage (r = 0.467) and disability (R = 0.200). The combination of first-line therapies led to reduced disability progression (r = 0.773), while second-line therapies resulted in improved overall axonal damage (r = 0.467).
Axonal damage occurs early and is the main cause of clinical disabilities. Prompt initiation of therapy is crucial to prevent axonal damage and thereby disability progression. A comprehensive therapeutic approach, including a combination of first- or second-line therapies, may improve long-term outcomes.
慢性炎症性脱髓鞘性多发性神经病(CIDP)的诊断可能具有挑战性,导致治疗开始延迟。由于CIDP中的残疾主要取决于轴突损伤,延迟免疫治疗的影响仍不清楚。我们采用多模式方法研究了早期CIDP患者在不同治疗策略和时间点的临床结局。
从前瞻性免疫介导神经病生物样本库(INHIBIT)登记处系统选取在纳入研究前1年内确诊为CIDP的患者。在纳入时和12个月后,对临床和治疗数据、神经传导研究(NCS)结果以及神经和肌肉超声检查结果进行关联分析。比较免疫治疗之间的患者结局。使用回归分析确定免疫治疗时机对临床结局的影响。
共纳入30例患者(从诊断到纳入的时间为22±19周)。复合肌肉动作电位低波幅与病理性自发电活动(PSA,r = 0.467)显著相关,并与赫克马特量表相关(r = 0.391)。所有这三个参数均与更高的总体残疾总分显著相关(NCS评分r = 0.581,PSA r = 0.385,赫克马特量表r = 0.472)。治疗开始延迟导致轴突损伤进展(r = 0.467)和残疾(R = 0.200)。一线治疗联合使用可减少残疾进展(r = 0.773),而二线治疗可改善总体轴突损伤(r = 0.467)。
轴突损伤早期发生,是临床残疾的主要原因。及时开始治疗对于预防轴突损伤从而防止残疾进展至关重要。包括一线或二线治疗联合使用的综合治疗方法可能会改善长期结局。