Department of Neurology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark.
Department of Clinical Neurophysiology, Rigshospitalet and Department of Neuroscience, University of Copenhagen, Copenhagen, Denmark.
Muscle Nerve. 2022 Dec;66(6):715-722. doi: 10.1002/mus.27722. Epub 2022 Oct 26.
INTRODUCTION/AIMS: We hypothesized that early, pretreatment axonal loss would predict long-term disability, supported by a pilot study of selected patients with chronic inflammatory demyelinating polyneuropathy (CIDP). To further test this hypothesis, we examined a larger consecutive group of CIDP patients.
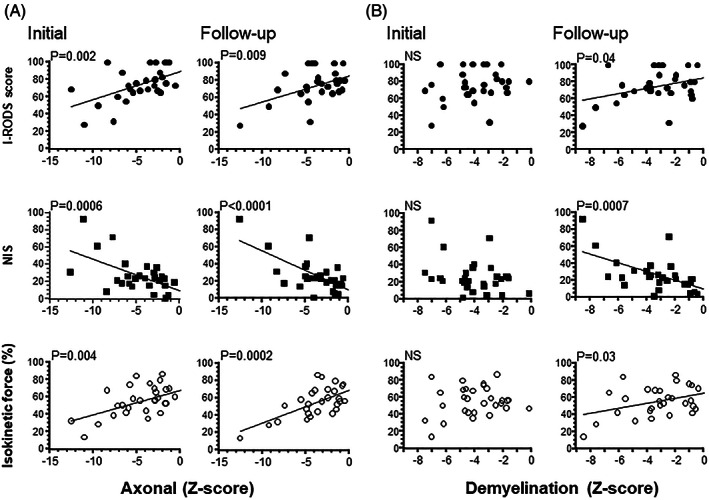
Needle electromyography and motor and sensory nerve conduction studies were carried out in 30 CIDP patients at pretreatment and follow-up 5 to 28 years later. Changes in amplitudes were expressed as axonal Z scores and changes in conduction as demyelination Z scores and correlated with findings of the Inflammatory Rasch-built Overall Disability Scale (I-RODS), the Neuropathy Impairment Score (NIS), and isokinetic dynamometry (IKS).
At follow-up, the median I-RODS score was 73, the NIS was 23, and the IKS was 56%. The median axonal Z score was unchanged at follow-up. Conversely, the corresponding demyelination Z scores improved. The initial axonal loss was correlated with the clinical outcome and was an independent predictor of outcome by multivariate regression analysis. Axonal loss at follow-up was also correlated with the clinical outcome. Only the follow-up demyelination Z score was correlated with the clinical outcomes. Furthermore, the latency until treatment initiation was predictive of all three clinical outcome scores at follow-up, and of axonal loss and demyelination at follow-up.
The present study findings indicate that pretreatment axonal loss at diagnosis in CIDP is predictive of long-term disability, neurological impairment, and strength. A delay in treatment is associated with more pronounced axonal loss and a worse clinical outcome.
简介/目的:我们假设早期治疗前轴索丢失会预测长期残疾,这一假设得到了一项针对慢性炎症性脱髓鞘性多发性神经病(CIDP)患者的前瞻性研究的支持。为了进一步验证这一假设,我们检查了一组更大的连续 CIDP 患者。
对 30 例 CIDP 患者进行了电针肌电图和运动及感觉神经传导研究,在治疗前和 5 至 28 年后的随访中进行。振幅变化用轴突 Z 评分表示,传导变化用脱髓鞘 Z 评分表示,并与炎症 Rasch 构建的总体残疾量表(I-RODS)、神经病变损伤评分(NIS)和等速动力学(IKS)的结果相关。
随访时,I-RODS 评分中位数为 73,NIS 为 23,IKS 为 56%。随访时轴索 Z 评分中位数无变化。相反,相应的脱髓鞘 Z 评分有所改善。初始轴索丢失与临床结局相关,并且通过多元回归分析成为结局的独立预测因素。随访时的轴索丢失也与临床结局相关。只有随访时的脱髓鞘 Z 评分与临床结局相关。此外,治疗开始的潜伏期与随访时的所有三个临床结局评分以及随访时的轴索丢失和脱髓鞘相关。
本研究结果表明,CIDP 诊断时的治疗前轴索丢失是长期残疾、神经损伤和肌力的预测因素。治疗延迟与更明显的轴索丢失和更差的临床结局相关。