Kosmala Aleksander, Hasenauer Natalie, Serfling Sebastian E, Michalski Kerstin, Fröhlich Matthias, Dreher Niklas, Hartrampf Philipp E, Higuchi Takahiro, Buck Andreas K, Weich Alexander, Reiter Theresa, Werner Rudolf A
Department of Nuclear Medicine, University Hospital Würzburg, Würzburg, Germany.
Internal Medicine II, University Hospital Würzburg, Würzburg, Germany.
Theranostics. 2025 Jan 1;15(3):804-814. doi: 10.7150/thno.102910. eCollection 2025.
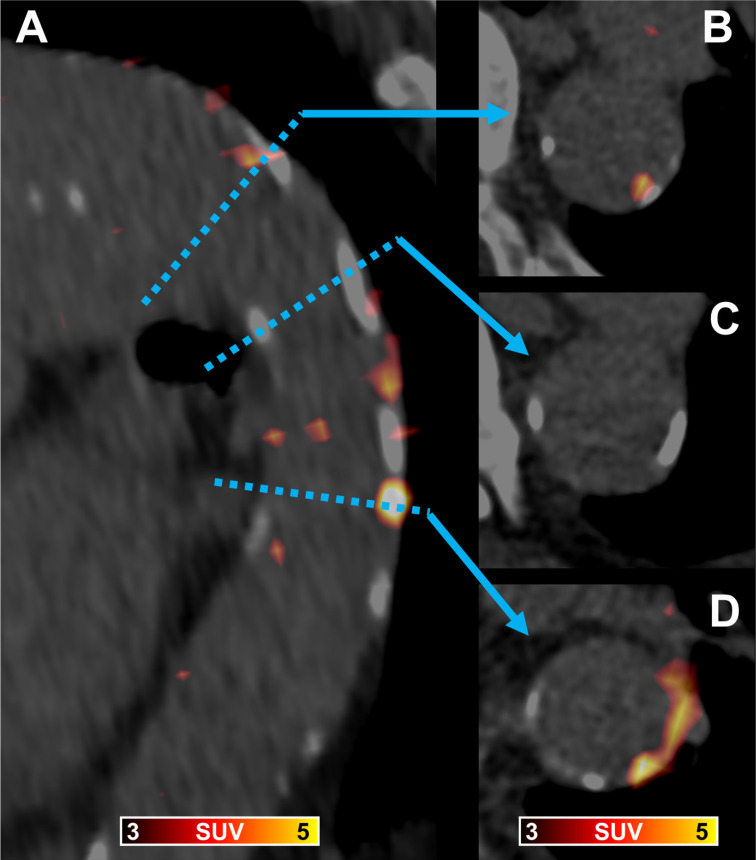
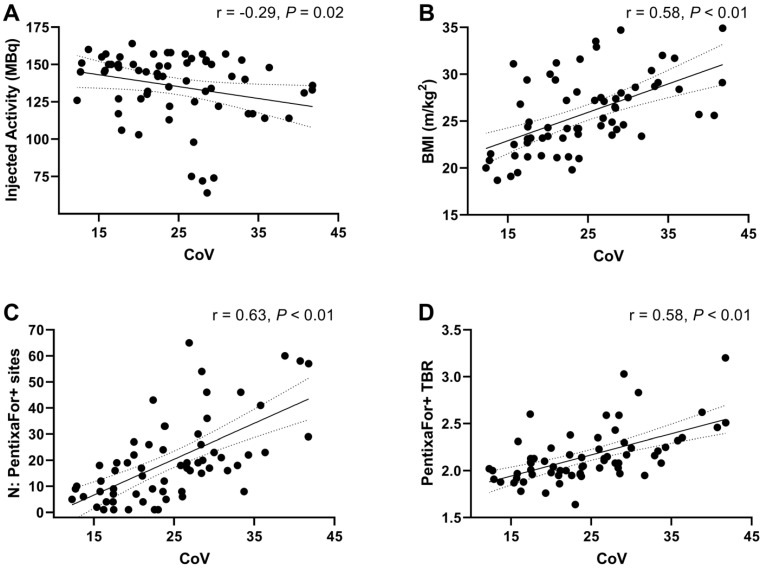
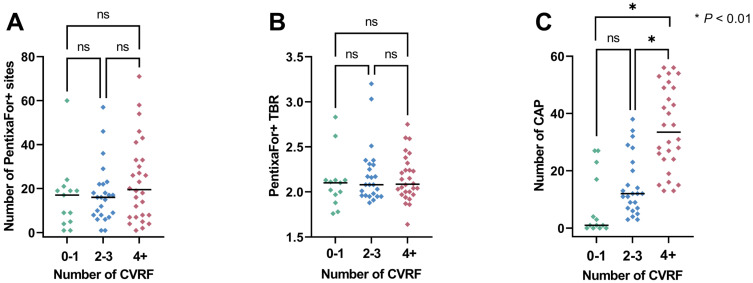
To establish the extent, distribution and frequency of in-vivo vessel wall [Ga]Ga-PentixaFor uptake and to determine its relationship with calcified atherosclerotic plaque burden (CAP) and cardiovascular risk factors (CVRF). 65 oncological patients undergoing [Ga]Ga-PentixaFor PET/CT were assessed. Radiotracer uptake (target-to-background ratio [TBR]) and CAP burden (including number of CAP sites, calcification circumference and thickness) in seven major vessel segments per patient were determined. We then investigated associations of vessel wall uptake with CAP burden, cardiovascular risk (CVRF and European Society of Cardiology [ESC] SCORE2/SCORE2-OP risk chart) and image noise (determined by coefficient of variation [CoV] from unaffected liver parenchyma). We identified 1292 sites of high focal [Ga]Ga-PentixaFor uptake (PentixaFor+ sites) in the vessel wall in 65/65 (100%) patients, with concomitant calcification in 385/1292 (29.8%) sites. There were no significant associations between vessel wall uptake and CAP burden (number of PentixaFor+ sites: r ≤ 0.18, ≥ 0.14; PentixaFor+ TBR: r ≤ 0.08, ≥ 0.54). The number of PentixaFor+ sites showed a moderate correlation with cardiovascular risk (ESC SCORE2/SCORE2-OP, r = 0.30; number of CVRF, r = 0.26; = 0.04, respectively), but failed to reach significance for PentixaFor+ TBR (r ≤ 0.18, ≥ 0.22). In univariable regression analysis, body mass index (odds ratio [OR] 1.08, 95%-confidence interval [CI] 1.02-1.14) and CoV (OR, 1.07; CI, 1.05-1.10) were linked to TBR and the number of PentixaFor+ sites ( < 0.01, respectively), while injected activity was only associated with the latter imaging parameter (OR, 0.99; CI, 0.98-1.00; = 0.04). In multivariable regression, injected activity (OR, 1.00; CI, 0.99-1.00) and CoV (OR, 1.06; CI, 1.06-1.07) remained significantly associated with the number of PentixaFor+ sites ( < 0.01, respectively). CoV, however, was the only parameter significantly linked to PentixaFor+ TBR on multivariable analysis (OR, 1.02; CI, 1.01-1.03; < 0.01). On a visual and quantitative level, high focal [Ga]Ga-PentixaFor uptake in the arterial tree was not consistently linked to vessel wall calcification or cardiovascular risk. Image noise, however, may account for a substantial portion of apparent vessel wall uptake.
确定体内血管壁[镓]镓-喷替酸五钠摄取的范围、分布和频率,并确定其与钙化动脉粥样硬化斑块负荷(CAP)和心血管危险因素(CVRF)的关系。对65例接受[镓]镓-喷替酸五钠PET/CT检查的肿瘤患者进行了评估。测定了每位患者七个主要血管节段的放射性示踪剂摄取(靶本底比[TBR])和CAP负荷(包括CAP部位数量、钙化周长和厚度)。然后,我们研究了血管壁摄取与CAP负荷、心血管风险(CVRF和欧洲心脏病学会[ESC]SCORE2/SCORE2-OP风险图表)以及图像噪声(由未受影响的肝实质的变异系数[CoV]确定)之间的关联。我们在65/65(100%)例患者的血管壁中确定了1292个[镓]镓-喷替酸五钠高摄取灶(喷替酸五钠阳性部位),其中385/1292(29.8%)个部位伴有钙化。血管壁摄取与CAP负荷之间无显著关联(喷替酸五钠阳性部位数量:r≤0.18,P≥0.14;喷替酸五钠阳性TBR:r≤0.08,P≥0.54)。喷替酸五钠阳性部位数量与心血管风险呈中度相关(ESC SCORE2/SCORE2-OP,r = 0.30;CVRF数量,r = 0.26;P分别为0.04),但喷替酸五钠阳性TBR未达到显著水平(r≤0.18,P≥0.22)。在单变量回归分析中,体重指数(优势比[OR]1.08,95%置信区间[CI]1.02 - 1.14)和CoV(OR,1.07;CI,1.05 - 1.10)与TBR和喷替酸五钠阳性部位数量相关(P均<0.01),而注射剂量仅与后一成像参数相关(OR,0.99;CI,0.98 - 1.00;P = 0.04)。在多变量回归中,注射剂量(OR,1.00;CI,0.99 - 1.00)和CoV(OR,1.06;CI,1.06 - 1.07)仍然与喷替酸五钠阳性部位数量显著相关(P均<0.01)。然而,在多变量分析中,CoV是与喷替酸五钠阳性TBR唯一显著相关的参数(OR,1.02;CI,1.01 - 1.03;P<0.01)。在视觉和定量水平上,动脉树中[镓]镓-喷替酸五钠的高摄取灶与血管壁钙化或心血管风险并无一致关联。然而,图像噪声可能在很大程度上解释了血管壁的表观摄取。