Rosen Jake L, Vemuri Siddharth, Rame J Eduardo, Rajapreyar Indranee N, Bermudez Christian A, Plestis Konstadinos A, Rajagopal Keshava
Division of Cardiac Surgery, Department of Surgery, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, Pennsylvania.
Division of Cardiology, Department of Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, Pennsylvania.
Ann Thorac Surg Short Rep. 2023 Dec 9;2(1):44-47. doi: 10.1016/j.atssr.2023.11.020. eCollection 2024 Mar.
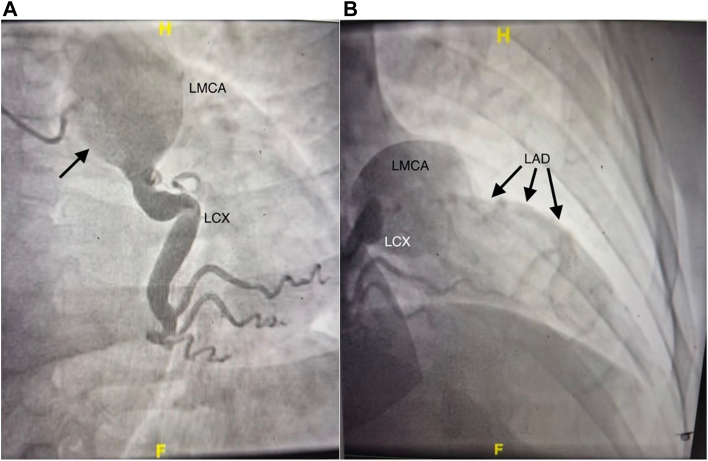
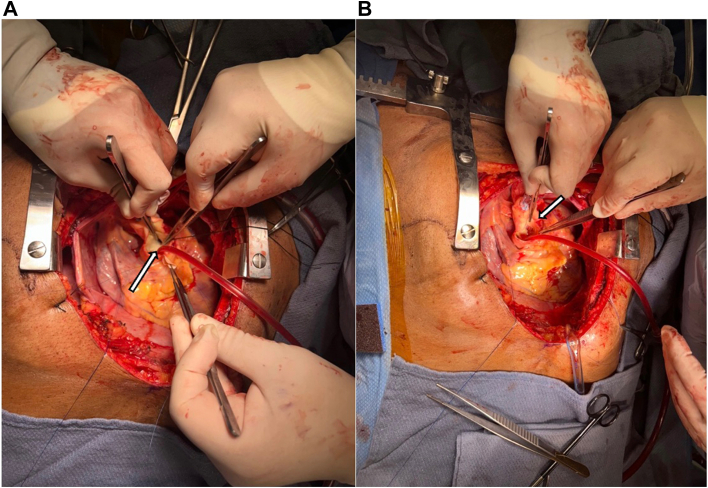
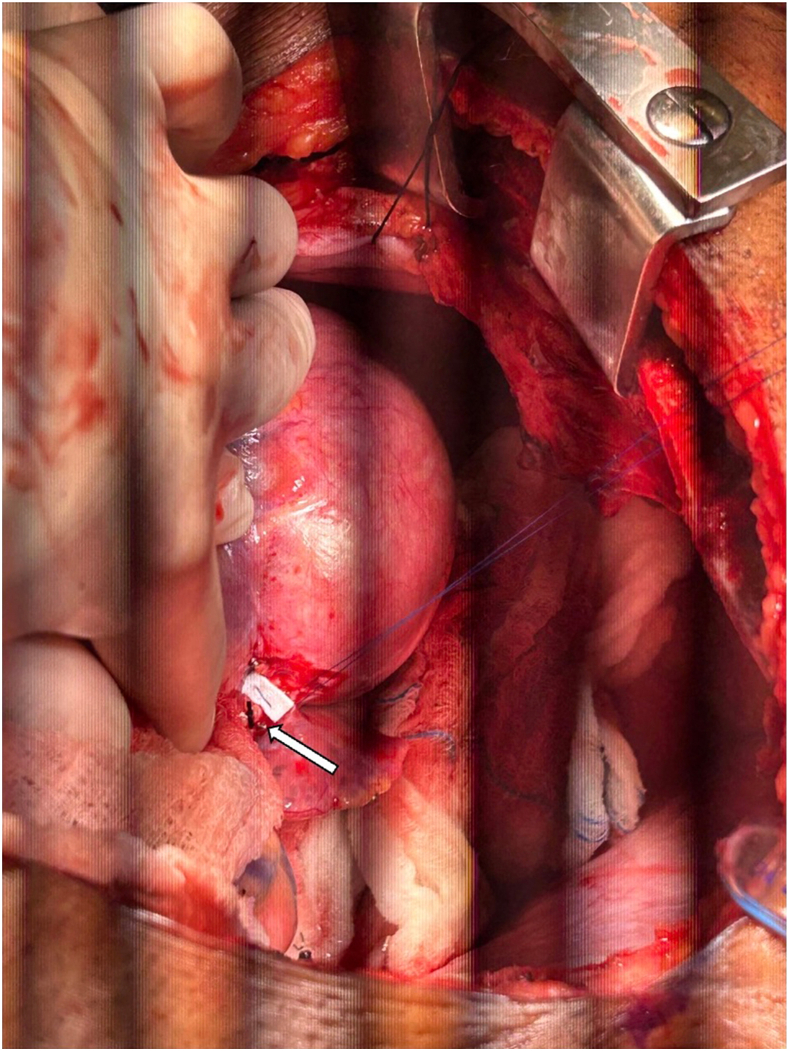
A 57-year-old man with a known left main coronary artery aneurysm presented with acutely decompensated heart failure and ventricular tachycardia secondary to ST elevation myocardial infarction. Transthoracic echocardiography identified a left ventricular ejection fraction <20% and anterior/septal wall akinesis. Left-sided cardiac catheterization revealed left anterior descending coronary artery occlusion. After the patient was placed on extracorporeal membrane oxygenation, delayed left ventricular distention developed, requiring further surgical intervention. Because of immense size, a novel "no-touch" approach was taken to the left main coronary artery aneurysm; the patient concomitantly underwent ventricular tachycardia ablation and continuous-flow left ventricular assist device implantation.
一名57岁男性,已知患有左主干冠状动脉瘤,因ST段抬高型心肌梗死继发急性失代偿性心力衰竭和室性心动过速入院。经胸超声心动图显示左心室射血分数<20%,前壁/室间隔运动不能。左侧心导管检查显示左前降支冠状动脉闭塞。患者接受体外膜肺氧合治疗后,出现延迟性左心室扩张,需要进一步手术干预。由于动脉瘤巨大,对左主干冠状动脉瘤采用了一种新颖的“非接触式”方法;患者同时接受了室性心动过速消融和连续流左心室辅助装置植入术。