Ishihara Shunta, Shimomura Masanori, Tsunezuka Hiroaki, Okada Satoru, Furuya Tatsuo, Yoshikawa Tatsuya, Inoue Masayoshi
Division of Thoracic Surgery, Department of Surgery, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Kyoto, Japan.
Department of Thoracic Surgery, Otsu City Hospital, Shiga, Japan.
Ann Thorac Surg Short Rep. 2024 May 27;2(4):608-612. doi: 10.1016/j.atssr.2024.04.032. eCollection 2024 Dec.
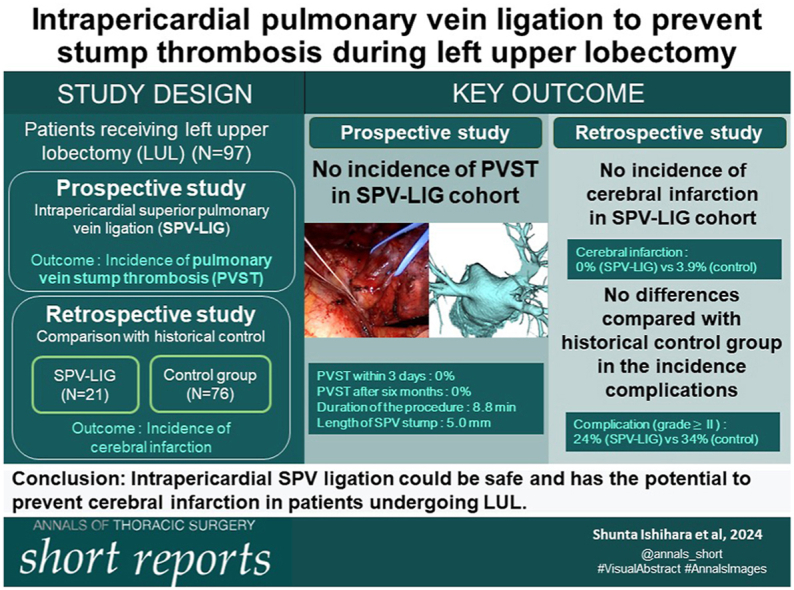
Postoperative cerebral infarction, a serious complication of surgery, is occasionally experienced with pulmonary vein stump thrombosis (PVST), which is frequently observed after left upper lobectomy (LUL). Herein, we prospectively investigated whether PVST could be safely prevented by intrapericardial ligation of the superior pulmonary vein (SPV) to shorten the SPV stump during LUL.
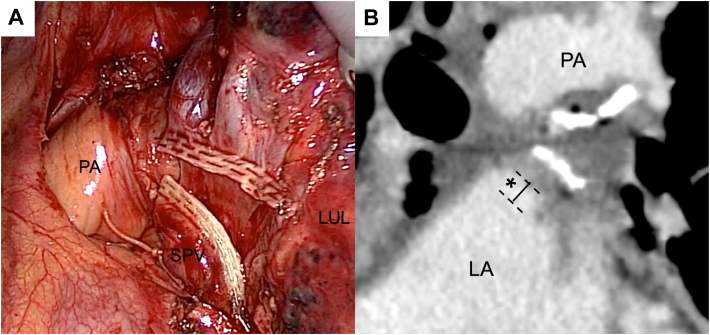
In a consecutive 21 patients who underwent LUL, we ligated the proximal intrapericardial SPV with 1-0 silk suture and divided the distal hilar SPV by an automatic stapling device. We measured the SPV stump length from the left atrium to the point of ligation and evaluated the presence of PVST on postoperative computed tomography. The procedure time was measured as the time from pericardial treatment initiation to the distal SPV division. Furthermore, the safety of the procedure and postoperative complications were evaluated and compared with those of 76 historical control patients who underwent LUL without intrapericardial SPV ligation.
The median procedure time was 8.8 minutes, and the median blood loss was 3 g. The median length of the SPV stump after the procedure was 5.0 mm. The 30- and 90-day mortality rates were both 0% for patients who underwent LUL with SPV ligation. None of the patients in the SPV ligation group showed signs of PVST on postoperative contrast-enhanced computed tomography images or had cerebrovascular disease. No significant difference in postoperative complications was observed between the groups.
Intrapericardial SPV ligation is safe and has a potential to prevent cerebral infarction after LUL.
术后脑梗死是一种严重的手术并发症,偶尔会伴有肺静脉残端血栓形成(PVST),这在左上肺叶切除术后(LUL)很常见。在此,我们前瞻性地研究了在左上肺叶切除术中通过心包内结扎上肺静脉(SPV)以缩短SPV残端是否能安全预防PVST。
在连续21例行左上肺叶切除术的患者中,我们用1-0丝线在心包内结扎近端SPV,并使用自动吻合器切断肺门远端的SPV。我们测量了从左心房到结扎点的SPV残端长度,并通过术后计算机断层扫描评估PVST的存在情况。手术时间定义为从开始心包处理到切断远端SPV的时间。此外,评估了该手术的安全性和术后并发症,并与76例未进行心包内SPV结扎的左上肺叶切除术历史对照患者进行了比较。
中位手术时间为8.8分钟,中位失血量为3克。术后SPV残端的中位长度为5.0毫米。接受SPV结扎的左上肺叶切除术患者的30天和90天死亡率均为0%。SPV结扎组的患者在术后增强计算机断层扫描图像上均未显示PVST迹象,也没有脑血管疾病。两组之间术后并发症无显著差异。
心包内SPV结扎是安全的,并且有可能预防左上肺叶切除术后的脑梗死。