Brousseau Karine, Monette Leah, McIsaac Daniel I, Wherrett Christopher, Mallick Ranjeeta, Workneh Aklile, Ramsay Tim, Tinmouth Alan, Shaw Julie, Presseau Justin, Hallet Julie, Carrier François M, Fergusson Dean A, Martel Guillaume
Department of Surgery, The Ottawa Hospital, University of Ottawa, Ottawa, ON, Canada; Clinical Epidemiology Program, Ottawa Hospital Research Institute, Ottawa, ON, Canada.
Clinical Epidemiology Program, Ottawa Hospital Research Institute, Ottawa, ON, Canada; Department of Anesthesiology and Pain Medicine, The Ottawa Hospital, University of Ottawa, Ottawa, ON, Canada.
Br J Anaesth. 2025 Feb;134(2):341-349. doi: 10.1016/j.bja.2024.09.033. Epub 2025 Jan 9.
Point-of-care testing devices to measure haemoglobin (Hgb) frequently inform transfusion decision-making in surgery. This study aimed to examine their accuracy in surgery, focusing on Hgb concentrations of 60-100 g L, a range with higher potential for transfusion.
This was a prospective diagnostic cohort study focused on method comparison, conducted at two academic hospitals. Consecutive patients undergoing noncardiac surgery and requiring point-of-care Hgb measurements were eligible. Hgb concentrations from arterial and central venous blood samples were measured concurrently using three devices and compared with laboratory Hgb. The primary outcome was individual pairwise comparisons between point-of-care and laboratory Hgb values; agreement was determined based on a threshold of within 4 g L. The primary analysis consisted of computing limits of agreement.
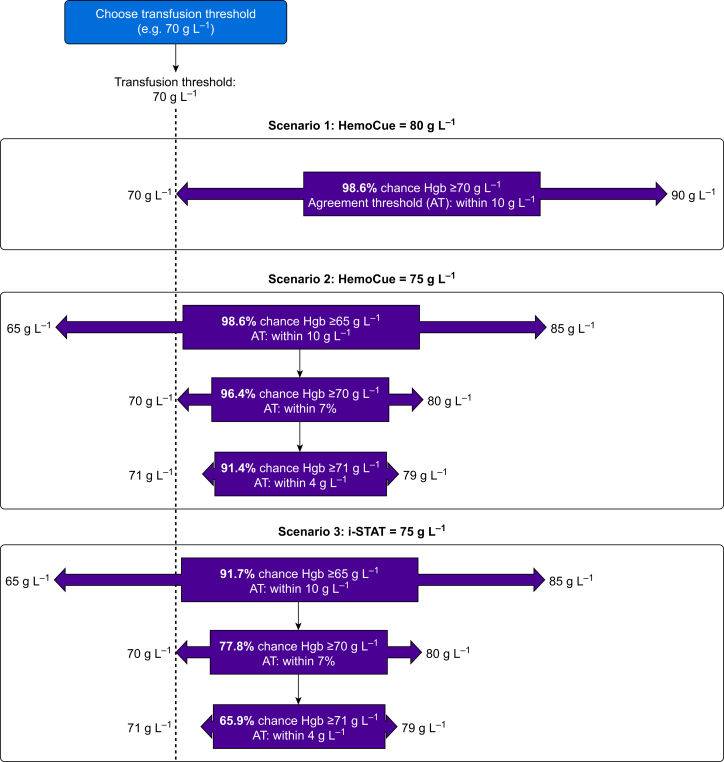
A total of 1735 intraoperative blood samples were collected (1139 participants); 680 samples had a laboratory Hgb <100 g L. The limits of agreement among those with Hgb <100 g L were -9.5 to 8.0 g L for HemoCue®, -16.2 to 11.5 g L for i-STAT®, and -14.7 to 40.5 g L for Rad-67®. HemoCue was associated with a 5.8% incidence of potentially clinically significant transfusion error, whereas i-STAT and Rad-67 were associated with 25.3% and 28.2%, respectively. HemoCue yielded Hgb measurements within 10 g L in 98% of intraoperative blood samples.
No point-of-care Hgb device demonstrated limits of agreement that were smaller than the agreement difference of 4 g L. Despite this, HemoCue can be safely used to inform transfusion decisions in surgery, given its error probability of <4% in transfusion scenarios.
用于测量血红蛋白(Hgb)的床旁检测设备常用于指导手术中的输血决策。本研究旨在检验其在手术中的准确性,重点关注血红蛋白浓度在60 - 100 g/L之间的情况,此范围输血可能性更高。
这是一项前瞻性诊断队列研究,重点在于方法比较,在两家学术医院进行。连续接受非心脏手术且需要进行床旁血红蛋白测量的患者符合条件。同时使用三种设备测量动脉血和中心静脉血样本中的血红蛋白浓度,并与实验室血红蛋白测量结果进行比较。主要结局是床旁血红蛋白值与实验室血红蛋白值的个体两两比较;根据4 g/L以内的阈值确定一致性。主要分析包括计算一致性界限。
共采集了1735份术中血样(1139名参与者);680份样本的实验室血红蛋白<100 g/L。对于HemoCue®,血红蛋白<100 g/L者的一致性界限为 - 9.5至8.0 g/L;对于i - STAT®为 - 16.2至11.5 g/L;对于Rad - 67®为 - 14.7至40.5 g/L。HemoCue与潜在临床显著输血误差发生率5.8%相关,而i - STAT和Rad - 67分别与25.3%和28.2%相关。在98%的术中血样中,HemoCue得出的血红蛋白测量值在10 g/L以内。
没有一种床旁血红蛋白检测设备的一致性界限小于4 g/L的一致性差异。尽管如此,鉴于HemoCue在输血情况下误差概率<4%,可安全用于指导手术中的输血决策。