Liu Timing, Sankareswaran Alagu, Paterson Gordon, Fraser Diane P, Hodgson Sam, Huang Qin Qin, Heng Teng Hiang, Ladwa Meera, Thomas Nick, van Heel David A, Weedon Michael N, Yajnik Chittaranjan S, Oram Richard A, Chandak Giriraj R, Martin Hilary C, Finer Sarah
Wellcome Trust Sanger Institute, Saffron Walden, UK.
Genomic Research on Complex diseases Group (GRC-Group), CSIR-Centre for Cellular and Molecular Biology, Hyderabad, India.
Sci Rep. 2025 Jan 13;15(1):1168. doi: 10.1038/s41598-024-80348-8.
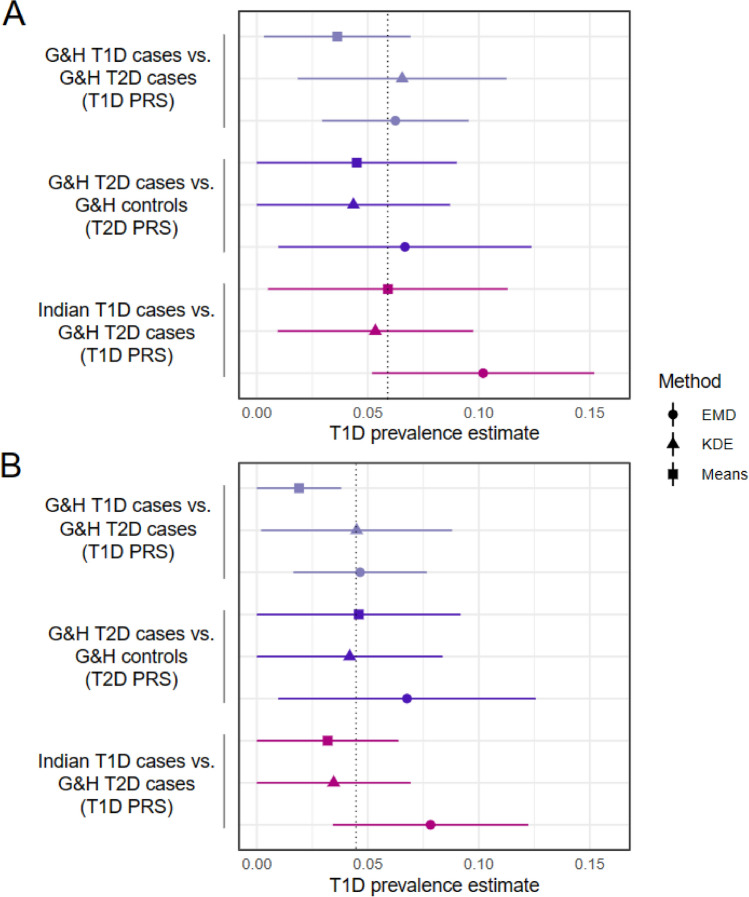
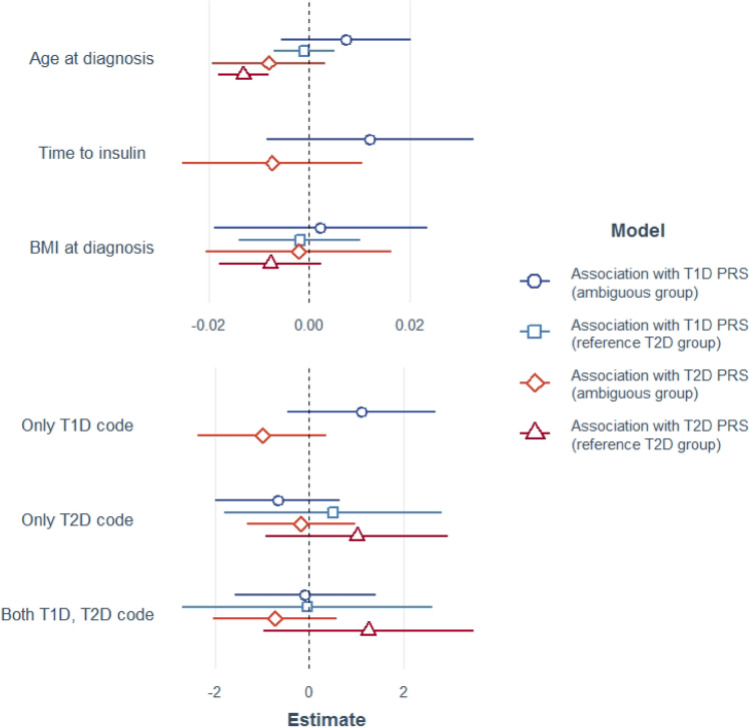
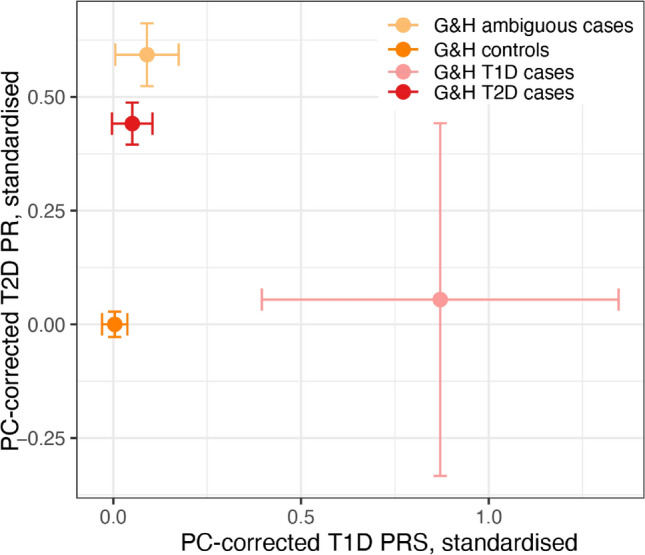
Correct classification of type 1 (T1D) and type 2 diabetes (T2D) is challenging due to overlapping clinical features and the increasingly early onset of T2D, particularly in South Asians. Polygenic risk scores (PRSs) for T1D and T2D have been shown to work relatively well in South Asians, despite being derived from largely European-ancestry samples. Here we used PRSs to investigate the rate of potential misclassification of diabetes amongst British Bangladeshis and Pakistanis. Using linked health records from the Genes & Health cohort (n = 38,344) we defined two reference groups meeting stringent diagnostic criteria: 31 T1D cases, 1842 T2D cases, and after excluding these, two further groups: 839 insulin-treated diabetic individuals with ambiguous features and 5174 non-diabetic controls. Combining these with 307 confirmed T1D cases and 307 controls from India, we calculated ancestry-corrected PRSs for T1D and T2D, with which we estimated the proportion of T1D cases within the ambiguous group at ~ 6%, dropping to ~ 4.5% within the subset who had T2D codes in their health records (and are thus most likely to have been misclassified). We saw no significant association between the T1D or T2D PRS and BMI at diagnosis, time to insulin, or the presence of T1D or T2D diagnostic codes amongst the T2D or ambiguous cases, suggesting that these clinical features are not particularly helpful for aiding diagnosis in ambiguous cases. Our results emphasise that robust identification of T1D cases and appropriate clinical care may require routine measurement of diabetes autoantibodies and C-peptide.
由于1型糖尿病(T1D)和2型糖尿病(T2D)的临床特征存在重叠,且T2D发病越来越早,尤其是在南亚人群中,因此对它们进行正确分类具有挑战性。尽管T1D和T2D的多基因风险评分(PRSs)主要来源于欧洲血统样本,但在南亚人群中已显示出相对较好的效果。在此,我们使用PRSs来研究英国孟加拉裔和巴基斯坦裔人群中糖尿病潜在误诊率。利用来自基因与健康队列(n = 38344)的关联健康记录,我们定义了两个符合严格诊断标准的参考组:31例T1D病例、1842例T2D病例,排除这些病例后,又定义了另外两组:839例具有模糊特征的接受胰岛素治疗的糖尿病个体和5174例非糖尿病对照。将这些与来自印度的307例确诊T1D病例和307例对照相结合,我们计算了T1D和T2D的血统校正PRSs,并据此估计了模糊组中T1D病例的比例约为6%,在健康记录中有T2D编码(因此最有可能被误诊)的子集中降至约4.5%。我们发现,在诊断时T1D或T2D PRS与体重指数、开始使用胰岛素的时间,或T2D或模糊病例中T1D或T2D诊断编码的存在之间没有显著关联,这表明这些临床特征对帮助诊断模糊病例并不是特别有用。我们的结果强调,要准确识别T1D病例并提供适当的临床护理,可能需要常规检测糖尿病自身抗体和C肽。