Chamié Daniel, Bahl Rahul, Maia Julio, Echavarria-Pinto Mauro, Gafore Suraya, Saleh Amr, Cristea Ecaterina, Seligman Henry, Joaquim Rodrigo M, Feres Fausto, Sen Sayan, Al-Lamee Rasha, Centemero Marinella, Baker Christopher, Johnson Tom, Shun-Shin Matthew J, Lansky Alexandra J, Petraco Ricardo
Section of Cardiovascular Medicine, Yale School of Medicine, New Haven, Connecticut.
Instituto Dante Pazzanese de Cardiologia, São Paulo, Brazil.
J Soc Cardiovasc Angiogr Interv. 2024 Oct 29;3(12):102396. doi: 10.1016/j.jscai.2024.102396. eCollection 2024 Dec.
The mechanistic association between the hydraulic forces generated during contrast injection and the risk of coronary injury is poorly understood. In this study, we sought to evaluate whether contrast injections increase intracoronary pressures beyond resting levels and estimate the risk of hydraulic propagation of coronary dissections.
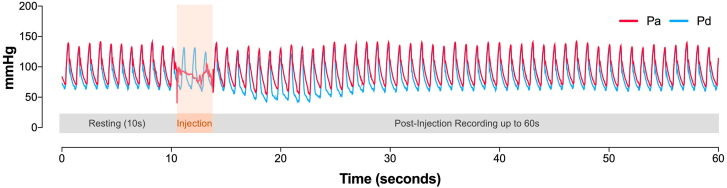
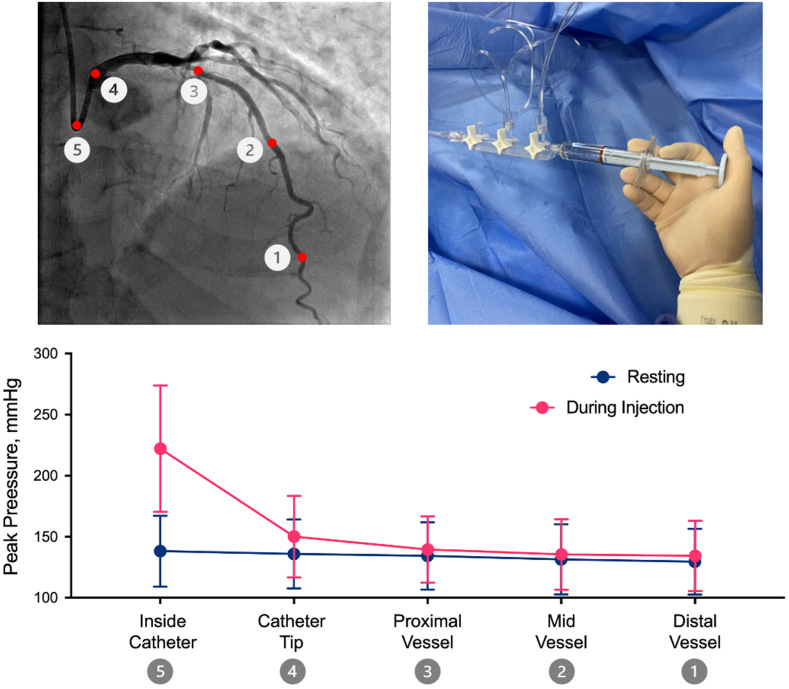
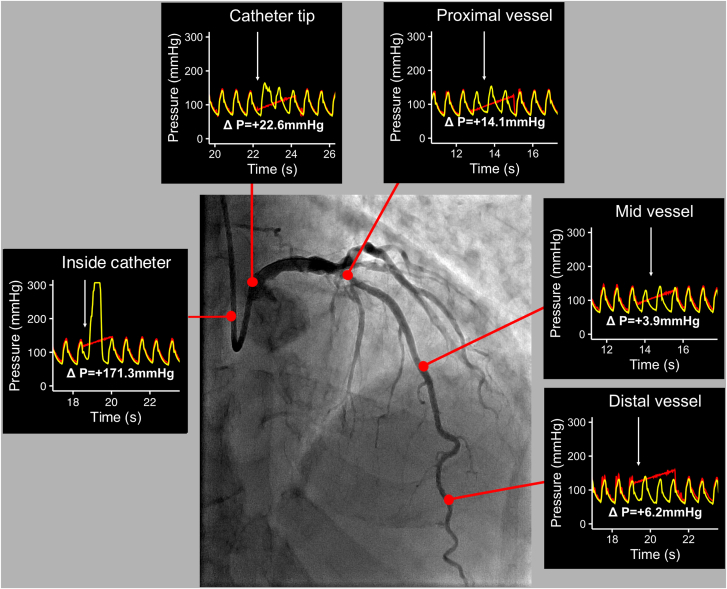
This is a prospective, single-arm, multicenter study that included patients with nonculprit, non-flow-limiting coronaries. A continuous 60-second pressure recording was taken at 5 predetermined locations during contrast injections: distal, mid, and proximal vessel, catheter tip, and inside the catheter. The primary end point was the change in intracoronary peak pressure between resting and injections in each location.
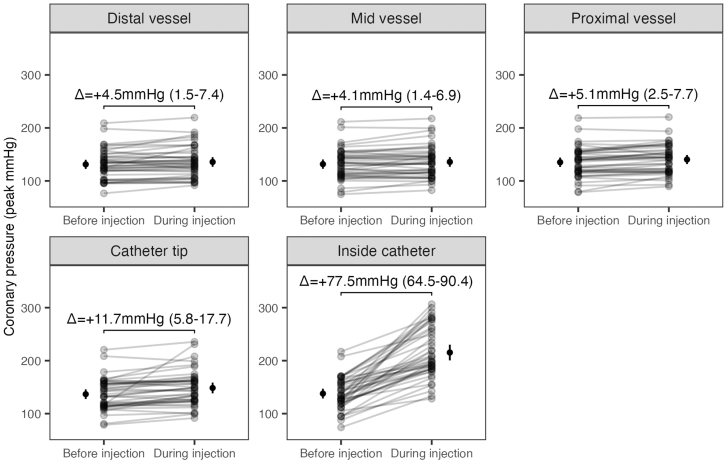
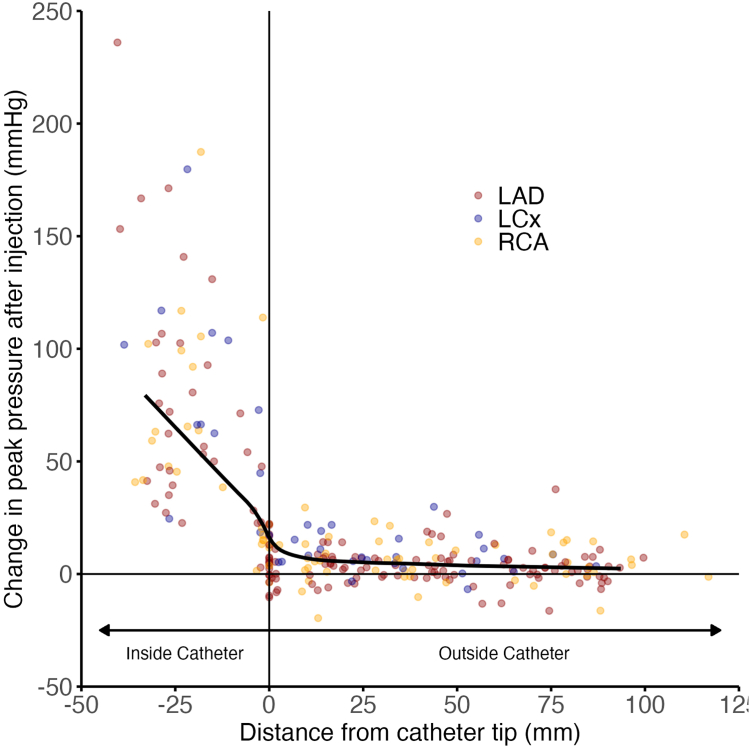
A total of 269 pressure recordings (58 vessels; 52 patients) were analyzed. Injections led to a small increase in peak pressure in the distal (mean difference, +4.5 mm Hg; 95% CI, 1.5-7.4), mid (mean difference, +4.1 mm Hg; 95% CI, 1.4-6.9), and proximal (mean difference, +5.1 mm Hg; 95% CI, 2.5-7.7) vessel locations, and much higher increases at the catheter tip (mean difference, +11.7 mm Hg; 95% CI, 5.8-17.7) and inside the catheter (mean difference, +77.5 mm Hg; 95% CI, 64.5-90.4). Compared to the distal vessel, pressure changes were only significant at the catheter tip (+10 mm Hg; < .01) and inside the catheter (+79.1 mm Hg; < .01).
Contrast injections lead to negligible changes in intracoronary pressures beyond the catheter tip. Although it is sensible to minimize injections when coronary dissections are close to the catheter, it is unlikely that they would cause injuries beyond the catheter tip.
在注射造影剂期间产生的液压与冠状动脉损伤风险之间的机制关联尚不清楚。在本研究中,我们试图评估造影剂注射是否会使冠状动脉内压力升高超过静息水平,并估计冠状动脉夹层液压传播的风险。
这是一项前瞻性、单臂、多中心研究,纳入了非罪犯、非血流限制性冠状动脉患者。在注射造影剂期间,于5个预定位置连续记录60秒压力:血管远端、中段、近端、导管尖端以及导管内部。主要终点是每个位置静息和注射期间冠状动脉内峰值压力的变化。
共分析了269次压力记录(58条血管;52例患者)。注射导致血管远端(平均差值,+4.5 mmHg;95%置信区间,1.5 - 7.4)、中段(平均差值,+4.1 mmHg;95%置信区间,1.4 - 6.9)和近端(平均差值,+5.1 mmHg;95%置信区间,2.5 - 7.7)位置的峰值压力小幅升高,而在导管尖端(平均差值,+11.7 mmHg;95%置信区间,5.8 - 17.7)和导管内部(平均差值,+77.5 mmHg;95%置信区间,64.5 - 90.4)升高幅度大得多。与血管远端相比,压力变化仅在导管尖端(+10 mmHg;P <.01)和导管内部(+79.1 mmHg;P <.01)显著。
造影剂注射导致导管尖端以外冠状动脉内压力变化可忽略不计。虽然当冠状动脉夹层靠近导管时尽量减少注射是合理的,但它们不太可能导致导管尖端以外的损伤。