Hodgkiss Daniel D, Balthazaar Shane J T, Welch Joseph F, Wadley Alex J, Cox Phoebe A, Lucas Rebekah A I, Veldhuijzen van Zanten Jet J C S, Chiou Shin-Yi, Lucas Samuel J E, Nightingale Tom E
School of Sport, Exercise and Rehabilitation Sciences, University of Birmingham, Birmingham, UK.
International Collaboration On Repair Discoveries, The University of British Columbia, Vancouver, British Columbia, Canada.
BMJ Open. 2025 Jan 15;15(1):e089756. doi: 10.1136/bmjopen-2024-089756.
Individuals with higher neurological levels of spinal cord injury (SCI) at or above the sixth thoracic segment (≥T6), exhibit impaired resting cardiovascular control and responses during upper-body exercise. Over time, impaired cardiovascular control predisposes individuals to lower cardiorespiratory fitness and thus a greater risk for cardiovascular disease and mortality. Non-invasive transcutaneous spinal cord stimulation (TSCS) has been shown to modulate cardiovascular responses at rest in individuals with SCI, yet its effectiveness to enhance exercise performance acutely, or promote superior physiological adaptations to exercise following an intervention, in an adequately powered cohort is unknown. Therefore, this study aims to explore the efficacy of acute TSCS for restoring autonomic function at rest and during arm-crank exercise to exhaustion (AIM 1) and investigate its longer-term impact on cardiorespiratory fitness and its concomitant benefits on cardiometabolic health and health-related quality of life (HRQoL) outcomes following an 8-week exercise intervention (AIM 2).
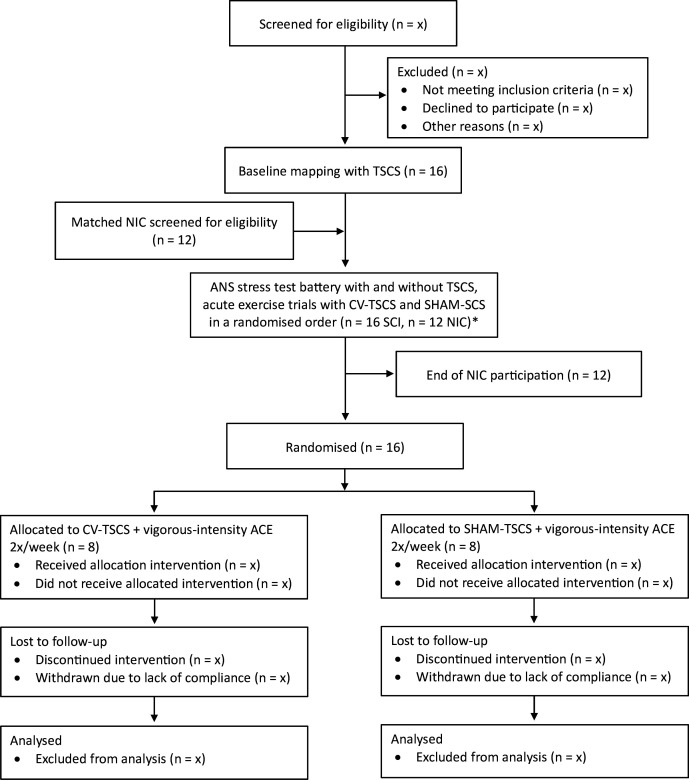
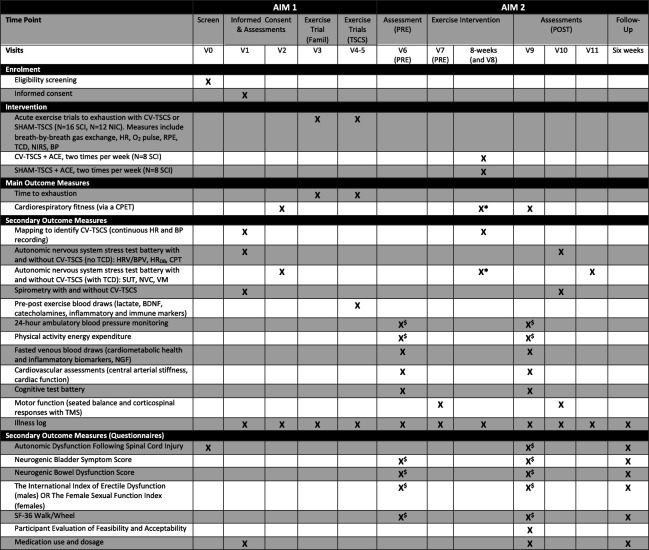
Sixteen individuals aged ≥16 years with a chronic, motor-complete SCI between the fifth cervical and sixth thoracic segments will undergo a baseline TSCS mapping session followed by an autonomic nervous system (ANS) stress test battery, with and without cardiovascular-optimised TSCS (CV-TSCS). Participants will then perform acute, single-session arm-crank exercise (ACE) trials to exhaustion with CV-TSCS or sham TSCS (SHAM-TSCS) in a randomised order. Twelve healthy, age- and sex-matched non-injured control participants will be recruited and will undergo the same ANS tests and exercise trials but without TSCS. Thereafter, the SCI cohort will be randomly assigned to an experimental (CV-TSCS+ACE) or control (SHAM-TSCS+ACE) group. All participants will perform 48 min of ACE twice per week (at workloads corresponding to 73-79% peak oxygen uptake), over a period of 8 weeks, either with (CV-TSCS) or without (SHAM-TSCS) cardiovascular-optimised stimulation. The primary outcomes are time to exhaustion (AIM 1) and cardiorespiratory fitness (AIM 2). Secondary outcomes for AIM 1 include arterial blood pressure, respiratory function, cerebral blood velocity, skeletal muscle tissue oxygenation, along with concentrations of catecholamines, brain-derived neurotrophic factor and immune cell dynamics via venous blood sampling pre, post and 90 min post-exercise. Secondary outcomes for AIM 2 include cardiometabolic health biomarkers, cardiac function, arterial stiffness, 24-hour blood pressure lability, energy expenditure, respiratory function, neural drive to respiratory muscles, seated balance and HRQoL (eg, bowel, bladder and sexual function). Outcome measures will be assessed at baseline, pre-intervention, post-intervention and after a 6-week follow-up period (HRQoL questionnaires only).
Ethical approval has been obtained from the Wales Research Ethics Committee 7 (23/WA/0284; 03/11/2024). The recruitment process began in February 2024, with the first enrolment in July 2024. Recruitment is expected to be completed by January 2026. The results will be presented at international SCI and sport-medicine conferences and will be submitted for publication in peer-reviewed journals.
ISRCTN17856698.
脊髓损伤(SCI)神经平面在第六胸段及以上(≥T6)的个体,在进行上身运动时,静息心血管控制及反应受损。随着时间推移,心血管控制受损使个体心肺适能降低,从而增加患心血管疾病和死亡的风险。已表明,非侵入性经皮脊髓刺激(TSCS)可调节SCI个体的静息心血管反应,但其在足够样本量队列中急性增强运动表现,或在干预后促进对运动的更好生理适应的有效性尚不清楚。因此,本研究旨在探讨急性TSCS恢复静息及手臂曲柄运动至力竭时自主神经功能的疗效(目标1),并调查其在8周运动干预后对心肺适能的长期影响及其对心脏代谢健康和健康相关生活质量(HRQoL)结果的伴随益处(目标2)。
16名年龄≥16岁、慢性、运动完全性SCI且损伤平面在第五颈椎至第六胸段之间的个体,将先进行一次基线TSCS图谱绘制,随后进行自主神经系统(ANS)应激测试组,测试时分别施加和不施加心血管优化TSCS(CV - TSCS)。参与者随后将以随机顺序进行急性单节段手臂曲柄运动(ACE)试验至力竭,试验时分别施加CV - TSCS或假TSCS(SHAM - TSCS)。将招募12名年龄、性别匹配的健康未受伤对照参与者,他们将进行相同的ANS测试和运动试验,但不施加TSCS。此后,SCI队列将被随机分配到实验组(CV - TSCS + ACE)或对照组(SHAM - TSCS + ACE)。所有参与者将在8周内每周两次进行48分钟的ACE(运动强度对应73 - 79%的峰值摄氧量),运动时一组施加(CV - TSCS),另一组不施加(SHAM - TSCS)心血管优化刺激。主要结局指标为运动至力竭时间(目标1)和心肺适能(目标2)。目标1的次要结局指标包括动脉血压、呼吸功能、脑血流速度、骨骼肌组织氧合,以及运动前、运动后和运动后90分钟通过静脉血样检测的儿茶酚胺、脑源性神经营养因子浓度和免疫细胞动态。目标2的次要结局指标包括心脏代谢健康生物标志物、心脏功能、动脉僵硬度、24小时血压变异性、能量消耗、呼吸功能、呼吸肌神经驱动、坐位平衡和HRQoL(如肠道、膀胱和性功能)。结局指标将在基线、干预前、干预后以及6周随访期(仅HRQoL问卷)进行评估。
已获得威尔士研究伦理委员会7的伦理批准(23/WA/0284;2024年11月3日)。招募过程于2024年2月开始,首次入组于2024年7月。预计招募将于2026年1月完成。研究结果将在国际SCI和运动医学会议上展示,并将提交至同行评审期刊发表。
ISRCTN17856698