Mathur Piyush, Naylor Amanda J, Auron Moises, Beresian Jean, Tallman Alexandra, Griffith Allison, Seasholtz Kathleen, Manlapaz Mariel, Zacharyasz Katherine, Khatib Reem, Mishra Shreya, Haller Kathryn, Fraser Thomas, Holman Katherine
Department of Anesthesiology, Cleveland Clinic, Cleveland, OH.
Outcomes Research Consortium, Houston, TX.
Crit Care Explor. 2025 Jan 16;7(1):e1205. doi: 10.1097/CCE.0000000000001205. eCollection 2025 Jan.
The current definition of central line-associated bloodstream infection (CLABSI) may overestimate the true incidence of CLABSI as it is often unclear whether the bloodstream infection (BSI) is secondary to the central line or due to another infectious source.
We aimed to assess the prevalence and outcomes of central CLABSI at our institution, to identify opportunities for improvement, appropriately direct efforts for infection reduction, and identify gaps in the CLABSI definition and its application as a quality measure.
Retrospective cross-sectional study of patients identified to have a CLABSI in the period 2018-2022 cared for at the value-based purchasing (VBP) units of a 1200-bed tertiary care hospital located in Cleveland, OH. Each CLABSI episode was assessed for relationship with central venous catheter (CVC), suspected secondary source of BSI, mortality associated with the CLABSI hospital encounter, and availability of infectious disease physician or primary physician documentation of infectious source.
CLABSI episodes were classified as CVC related, CVC unrelated, and CVC relationship unclear. Mortality during the same encounter as the CLABSI event was assessed as an outcome measure. Descriptive statistics were performed.
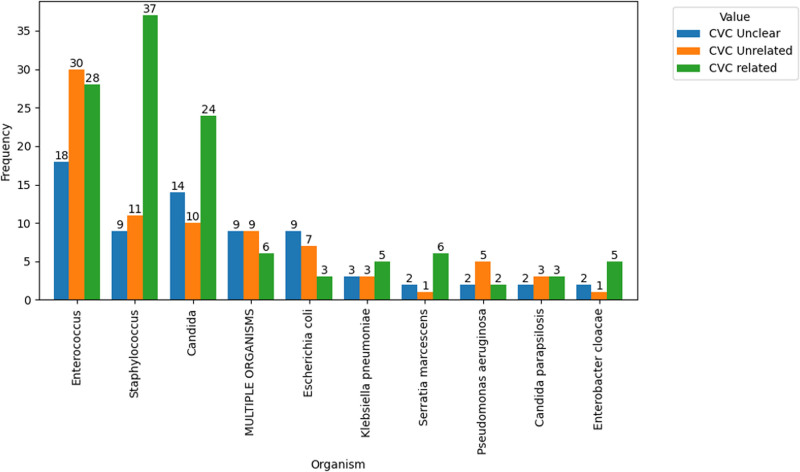
A total of 340 CLABSI episodes occurred in adult patients in VBP units. Majority of the CLABSI, 77.5% (266), occurred in the ICU. Of the CLABSI analyzed, 31.5% (107) were classified as unrelated to the CVC; 25.0% (85) had an unclear source; 43% (148) were classified as CVC related. For CVC-related cases, and were the predominant organisms. For the CVC unrelated and unclear groups was most prevalent. The mortality rate was lowest among patients classified with a CVC-related BSI. The positive predictive value (PPV) of the Centers for Disease Control and Prevention CLABSI definition to predict a true CVC-related infection was found to be 58.0%.
The definition of CLABSI as a surrogate for catheter-related BSI is inadequate, with a PPV of 58.0% (43.1-67.6%). Efforts should be redirected toward revising the CLABSI definition and possibly reevaluating its criteria. Resources should be assigned to further investigate and systematically prevent BSIs from secondary sources while adhering to existing CLABSI prevention bundles.
目前中心静脉导管相关血流感染(CLABSI)的定义可能高估了CLABSI的真实发病率,因为通常不清楚血流感染(BSI)是继发于中心静脉导管还是由其他感染源引起。
我们旨在评估我院中心CLABSI的患病率和结局,确定改进机会,合理指导降低感染的努力,并确定CLABSI定义及其作为质量指标应用中的差距。
设计、地点和参与者:对2018 - 2022年期间在俄亥俄州克利夫兰市一家拥有1200张床位的三级护理医院的价值购买(VBP)病房接受治疗且被确定患有CLABSI的患者进行回顾性横断面研究。评估每例CLABSI事件与中心静脉导管(CVC)的关系、疑似BSI的继发来源、与CLABSI住院相关的死亡率以及传染病医生或主治医生关于感染源的记录情况。
CLABSI事件分为与CVC相关、与CVC不相关以及与CVC关系不明确三类。将CLABSI事件发生期间的死亡率作为结局指标进行评估。进行描述性统计。
VBP病房的成年患者共发生340例CLABSI事件。大多数CLABSI事件(77.5%,266例)发生在重症监护病房(ICU)。在分析的CLABSI事件中,31.5%(107例)被归类为与CVC不相关;25.0%(85例)来源不明确;43%(148例)被归类为与CVC相关。对于与CVC相关的病例,[具体微生物名称1]和[具体微生物名称2]是主要病原体。对于与CVC不相关和来源不明确的组,[具体微生物名称3]最为常见。与CVC相关的BSI患者的死亡率最低。发现疾病控制与预防中心CLABSI定义预测真正与CVC相关感染的阳性预测值(PPV)为58.0%。
将CLABSI定义作为导管相关BSI的替代指标并不充分,PPV为58.0%(43.1 - 67.6%)。应重新调整努力方向,修订CLABSI定义并可能重新评估其标准。应分配资源进一步调查并系统预防继发来源的BSI,同时坚持现有的CLABSI预防措施。