Yang Xiaoming, Liu Zhongda, Liu Xiaojing, Li Quan, Huang Hui, Wei Yibo, Sun Tao
Department of Respiratory and Critical Care Medicine, Lishui Hospital of Traditional Chinese Medicine Affiliated to Zhejiang University of Traditional Chinese Medicine, No. 800 Zhongshan Road, Liandu District, Lishui, Zhejiang, 323000, China.
BMC Pulm Med. 2025 Jan 20;25(1):29. doi: 10.1186/s12890-025-03481-8.
Legionella pneumophila is an uncommon pathogen causing community-acquired atypical pneumonia. Acinetobacter baumannii is a major pathogen responsible for hospital-acquired pneumonia, but it rarely causes serious infections in a community setting. Without prompt and appropriate treatments, infection from either of these two pathogens can cause a high mortality rate. Concurrent infection from both L. pneumophila and A. baumannii can cause serious outcomes, but it has rarely been reported previously.
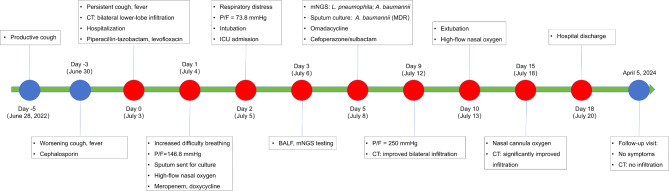
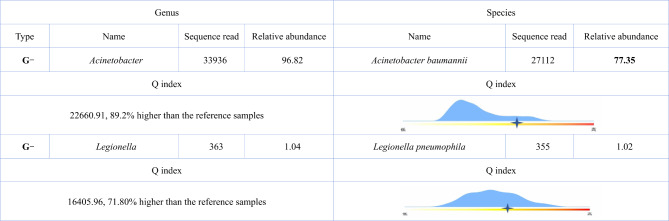
A 45-year-old male presented to our hospital with a productive cough and fever after staying in a local hotel. His chest computed tomography (CT) scan showed bilateral lower-lobe infiltration and left pleural effusion. Empirical antibiotics, including piperacillin-tazobactam, levofloxacin, meropenem, and doxycycline, were administered to him to treat community-acquired pneumonia. However, his condition deteriorated very rapidly, and he required endotracheal intubation and mechanical ventilation for respiratory support. Finally, metagenomic next-generation sequencing (mNGS) of his bronchoalveolar lavage fluid identified L. pneumophila and A. baumannii. The sputum culture demonstrated multidrug-resistant A. baumannii. He was diagnosed with pneumonia by concurrent infections from both L. pneumophila and A. baumannii. After careful consideration of the antibiotic susceptibility results and the antibacterial mechanism of each antibiotic, we switched the antibiotics to omadacycline and cefoperazone/sulbactam. His clinical symptoms gradually subsided. The repeat chest CT image showed no infiltration or pleural effusion.
Community-acquired pneumonia can be caused by concurrent infections of both L. pneumophila and A. baumannii. Close clinical monitoring, early pathogen detection and antibiotic susceptability tests, and appropriate antibiotic regimen adjustments should be applied to these patients who failed initial antibiotic treatments.
嗜肺军团菌是引起社区获得性非典型肺炎的一种不常见病原体。鲍曼不动杆菌是医院获得性肺炎的主要病原体,但在社区环境中很少引起严重感染。如果不及时进行适当治疗,这两种病原体中的任何一种感染都可能导致高死亡率。嗜肺军团菌和鲍曼不动杆菌的合并感染可导致严重后果,但此前鲜有报道。
一名45岁男性在入住当地一家酒店后,因咳嗽咳痰和发热前来我院就诊。他的胸部计算机断层扫描(CT)显示双侧下叶浸润及左侧胸腔积液。给予他包括哌拉西林-他唑巴坦、左氧氟沙星、美罗培南和多西环素在内的经验性抗生素治疗社区获得性肺炎。然而,他的病情迅速恶化,需要气管插管和机械通气以维持呼吸支持。最后,对他的支气管肺泡灌洗液进行宏基因组下一代测序(mNGS)鉴定出嗜肺军团菌和鲍曼不动杆菌。痰培养显示鲍曼不动杆菌对多种药物耐药。他被诊断为嗜肺军团菌和鲍曼不动杆菌合并感染所致的肺炎。在仔细考虑抗生素敏感性结果及每种抗生素的抗菌机制后,我们将抗生素更换为奥马环素和头孢哌酮/舒巴坦。他的临床症状逐渐消退。复查胸部CT图像显示无浸润或胸腔积液。
社区获得性肺炎可由嗜肺军团菌和鲍曼不动杆菌合并感染引起。对于初始抗生素治疗失败的患者,应密切进行临床监测、早期病原体检测和抗生素敏感性试验,并进行适当的抗生素方案调整。