Claahsen-van der Grinten Hedi L, Adriaansen Bas P H, Falhammar Henrik
Department of Pediatrics, Division of Pediatric Endocrinology, Amalia Children's Hospital, Radboud University Medical Center, 6500 HB Nijmegen, the Netherlands.
Department of Molecular Medicine and Surgery, Karolinska Institutet, 171 76 Stockholm, Sweden.
J Clin Endocrinol Metab. 2025 Jan 21;110(Supplement_1):S25-S36. doi: 10.1210/clinem/dgae718.
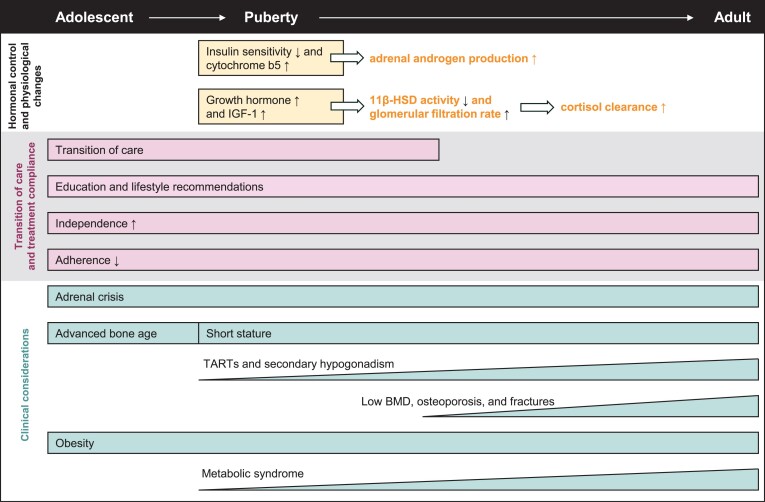
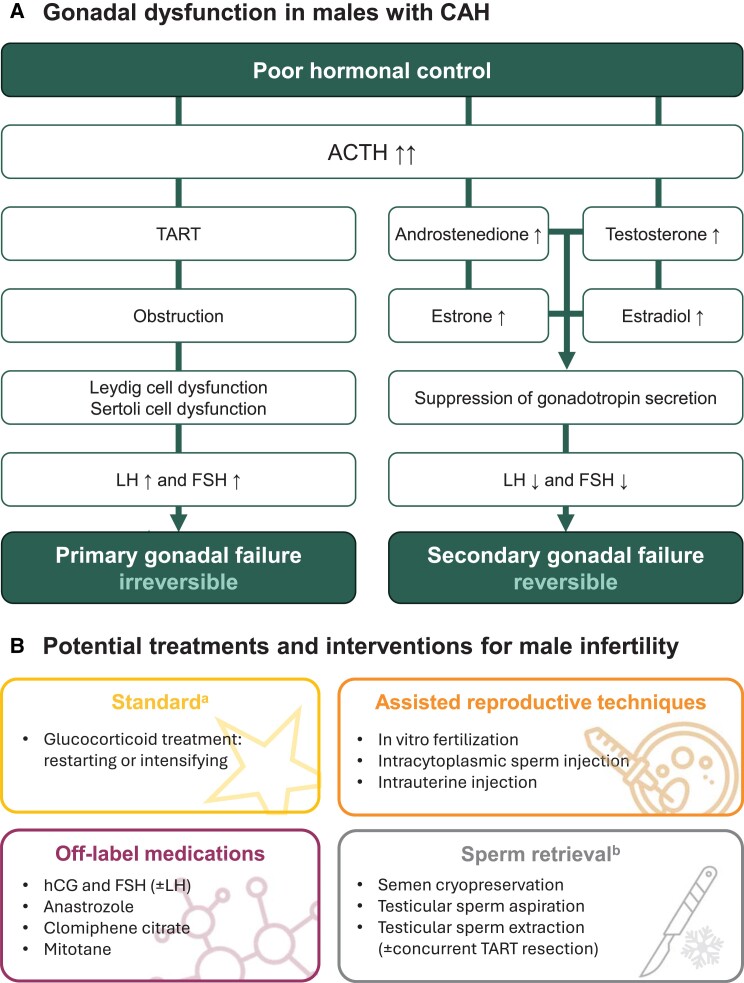
Classic congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency results in severe cortisol and aldosterone deficiency, leading to persistent adrenal stimulation and excess production of ACTH and adrenal androgens. This review examines the clinical considerations and challenges of balancing under- and overtreatment with glucocorticoids in adolescent and adult male individuals with CAH. Adolescents face many unique challenges that can hinder adherence, hormonal control, and transition to independence. Thus, patient education is critical during adolescence, especially in poorly controlled postpubertal males who lack obvious symptoms and may not recognize the long-term consequences of nonadherence, such as reduced final height, reduced reproductive health, poor bone health, obesity, and hypertension. The risk of subfertility/infertility begins early, especially in males with poor hormonal control, who often have reduced sperm counts, small testes, and benign tumors called testicular adrenal rest tumors (TARTs). Even males with good hormonal control can experience subfertility/infertility due to TARTs. In addition, several factors such as hypogonadism and long-term glucocorticoid treatment can predispose males with CAH to poor bone health (eg, low bone mineral density, increased risk of osteoporosis/osteopenia and fractures) and metabolic syndrome (eg, obesity, insulin resistance, dyslipidemia, and hypertension). Regular monitoring is recommended, with glucocorticoid dose optimization and prophylactic treatment to maximize future fertility potential and protect long-term bone health. Early implementation of lifestyle interventions and medical treatment are needed to address cardiometabolic consequences.
由21-羟化酶缺乏引起的经典型先天性肾上腺皮质增生症(CAH)会导致严重的皮质醇和醛固酮缺乏,进而导致肾上腺持续受到刺激,促肾上腺皮质激素(ACTH)以及肾上腺雄激素分泌过多。本综述探讨了在患有CAH的青少年和成年男性中,平衡糖皮质激素不足治疗和过度治疗的临床考量及挑战。青少年面临许多独特的挑战,这些挑战可能会妨碍其依从性、激素控制以及向独立的过渡。因此,青春期的患者教育至关重要,尤其是对于青春期后控制不佳、缺乏明显症状且可能未认识到不依从的长期后果(如最终身高降低、生殖健康受损、骨骼健康不佳、肥胖和高血压)的男性患者。生育力低下/不育的风险在早期就已出现,尤其是对于激素控制不佳的男性,他们通常精子数量减少、睾丸较小,并且会出现称为睾丸肾上腺残余肿瘤(TARTs)的良性肿瘤。即使是激素控制良好的男性也可能因TARTs而出现生育力低下/不育。此外,性腺功能减退和长期糖皮质激素治疗等多种因素可使患有CAH的男性易患骨骼健康不佳(如骨矿物质密度低、骨质疏松/骨质减少和骨折风险增加)和代谢综合征(如肥胖、胰岛素抵抗、血脂异常和高血压)。建议进行定期监测,优化糖皮质激素剂量并进行预防性治疗,以最大限度地提高未来生育潜力并保护长期骨骼健康。需要尽早实施生活方式干预和药物治疗,以应对心脏代谢方面的后果。