Neal Matthew D, Okonkwo David O, Guyette Francis X, Luther James F, Vincent Laura E, Puccio Ava M, Harner Ashley M, Agnone Allison G, Brubaker Donovan P, Love Emily T, Leeper Christine M, Brown Joshua B, Forsythe Raquel, Spinella Philip C, Yazer Mark H, Wisniewski Stephen R, Sperry Jason L
Department of Surgery, Trauma and Transfusion Medicine Research Center, University of Pittsburgh, Pittsburgh, PA.
Department of Neurological Surgery, University of Pittsburgh, Pittsburgh, PA.
Ann Surg. 2025 May 1;281(5):796-805. doi: 10.1097/SLA.0000000000006640. Epub 2025 Jan 22.
To determine the feasibility, efficacy, and safety of cold storage compared with room temperature (RT) platelet transfusion in patients with traumatic brain injury (TBI).
Data demonstrating the safety and efficacy of cold-stored platelet (CSP) transfusion are lacking after TBI.
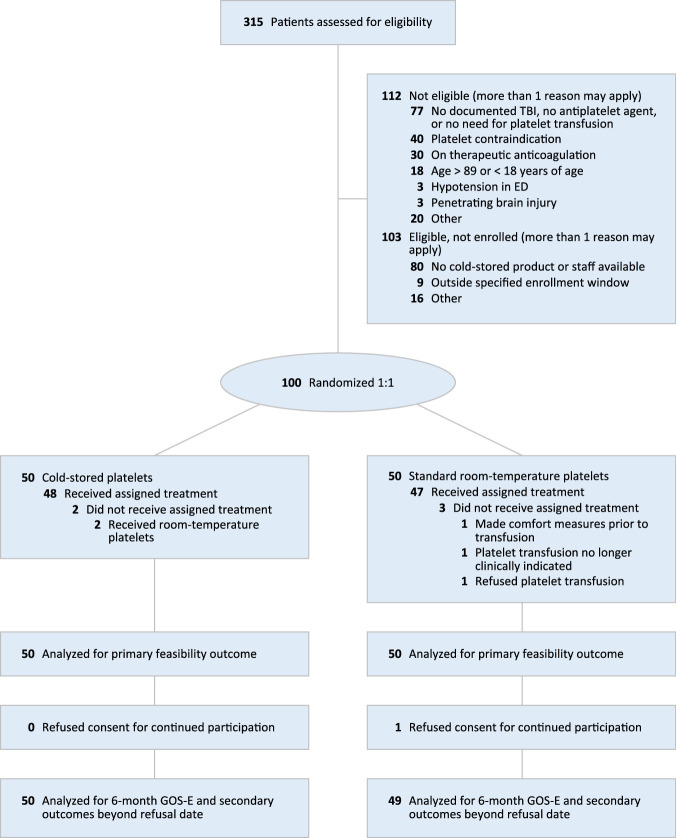
A phase 2, randomized, open-label clinical trial was performed at a single U.S. trauma center. Traumatic brain-injured patients with positive brain imaging and a need for platelet transfusion received up to 2 apheresis units of CSPs stored out to 14 days versus standard care RT platelet transfusion. The primary outcome was feasibility and the principal clinical outcome for efficacy and safety was the 6-month Glasgow Coma Scale-extended score.
The 6-month Glasgow Outcome Scale-extended score distributions were not different across cold stored and RT platelet arms (odds ratio: 1.58, 95% CI: 0.71 to 3.54, P = 0.27). A lower rate of neurosurgical craniotomy/craniectomy was found for those receiving CSPs (difference: -14.4%, 95% CI: -26.5% to -2.3%, P = 0.03). Adverse event rates did not differ across groups. The storage age of the cold-stored product was not associated with outcome differences.
In brain-injured patients requiring platelet transfusion, early CSP transfusion is feasible and did not result in improved 6-month Glasgow Coma Scale-extended scores. Early CSP transfusion was associated with a lower rate of neurosurgical operative intervention without an increase in adverse events. The storage age of the CSP product was not associated with outcome differences. Future phase 3 clinical trials are required to determine clinical outcome differences and safety attributable to CSP transfusion after TBI.
确定与室温(RT)血小板输注相比,冷藏血小板输注用于创伤性脑损伤(TBI)患者的可行性、疗效和安全性。
TBI后缺乏证明冷藏血小板(CSP)输注安全性和疗效的数据。
在美国一家创伤中心进行了一项2期随机开放标签临床试验。脑成像阳性且需要血小板输注的创伤性脑损伤患者接受最多2个单采单位的CSP,储存时间长达14天,与标准护理RT血小板输注进行比较。主要结局是可行性,疗效和安全性的主要临床结局是6个月格拉斯哥昏迷量表扩展评分。
冷藏和RT血小板组的6个月格拉斯哥结局量表扩展评分分布无差异(优势比:1.58,95%CI:0.71至3.54,P = 0.27)。接受CSP的患者进行神经外科开颅/颅骨切除术的发生率较低(差异:-14.4%,95%CI:-26.5%至-2.3%,P = 0.03)。各组不良事件发生率无差异。冷藏产品的储存时间与结局差异无关。
在需要血小板输注的脑损伤患者中,早期CSP输注是可行的,并且并未使6个月格拉斯哥昏迷量表扩展评分得到改善。早期CSP输注与较低的神经外科手术干预率相关,且不良事件未增加。CSP产品的储存时间与结局差异无关。未来需要进行3期临床试验,以确定TBI后CSP输注所致的临床结局差异和安全性。