Pylväläinen Juho, Talala Kirsi, Raitanen Jani, Rannikko Antti, Auvinen Anssi
Department of Radiology, HUS Diagnostic Centre, Helsinki University Hospital, Helsinki, Finland.
Research Program in Systems Oncology, Faculty of Medicine, University of Helsinki, Helsinki, Finland.
BJU Int. 2025 May;135(5):841-850. doi: 10.1111/bju.16641. Epub 2025 Jan 22.
To assess the association between prostate-specific antigen (PSA) density (PSAD) and prostate cancer mortality after a benign result on systematic transrectal ultrasonography (TRUS)-guided prostate biopsy.
This retrospective study used data from the Finnish Randomised Study of Screening for Prostate Cancer (FinRSPC) collected between 1996 and 2020. We identified men aged 55-71 years randomised to the screening arm with PSA ≥4.0 ng/mL and a benign systematic TRUS-guided biopsy result. The cumulative prostate cancer mortality of men stratified by a PSAD cutoff of 0.15 ng/mL/cm was modelled with competing risk functions. The ability of PSAD, PSA, and base variables (age at biopsy, DRE result, socioeconomic status, 5α-reductase inhibitor usage, family history, and Charlson Comorbidity Index (CCI)) to predict prostate cancer death was compared using c-statistics and a likelihood ratio test.
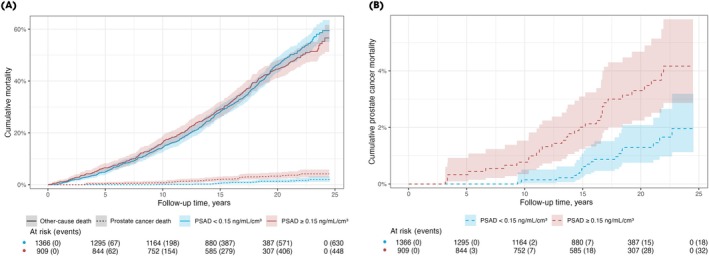
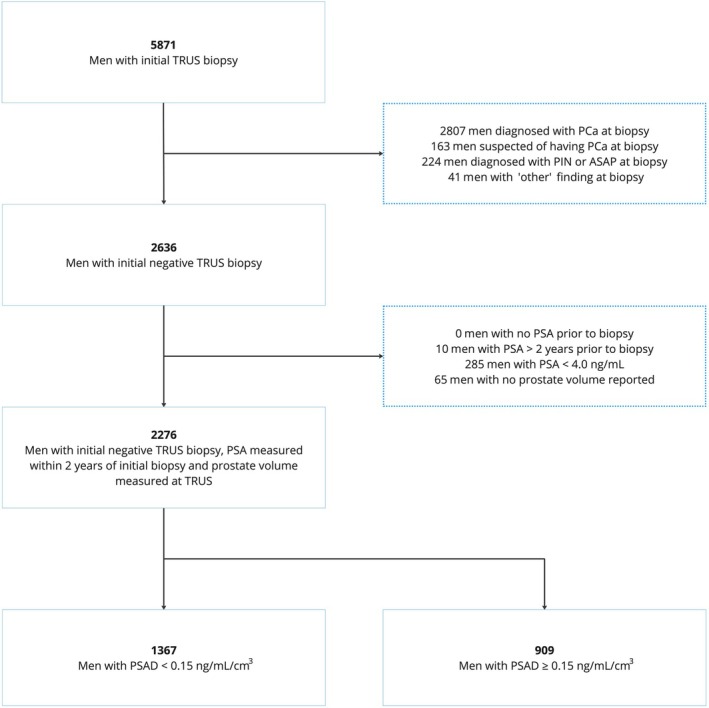
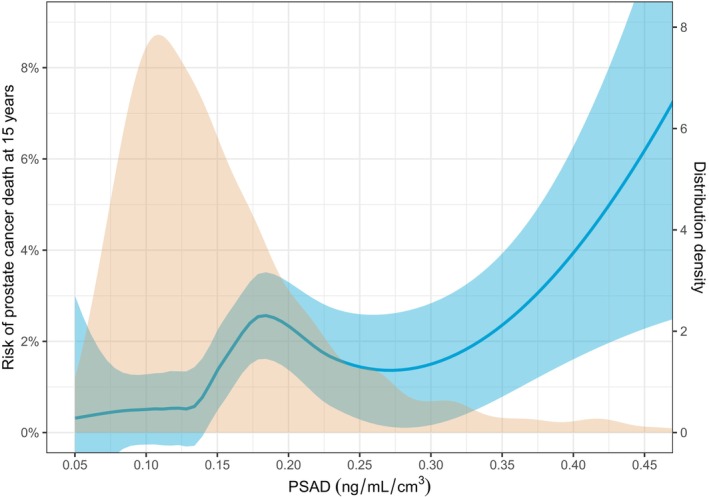
After excluding 10 men without PSA data within 2 years of the biopsy and 65 without prostate volume data, 2276 men were eligible for inclusion in the study. A total of 50 men died from prostate cancer and 1028 from other causes during a median (interquartile range) follow-up of 17.4 (13.2-20.9) years. The cumulative prostate cancer mortality of men with PSAD <0.15 ng/mL/cm was significantly lower than that of men with PSAD ≥0.15 ng/mL/cm: 0.5% (95% confidence interval [CI] 0.2%-1.1%) vs 2.0% (95% CI 1.2%-3.1%) at 15 years (Grey's test, P = 0.001). The model consisting of PSAD, PSA and the base variables predicted prostate cancer mortality (c-statistic 0.781) significantly better than either the base variables alone (c-statistic 0.737; likelihood-ratio test, P = 0.003) or the base variables and PSA (c-statistic 0.765; likelihood-ratio test, P = 0.039).
Prostate cancer mortality after a benign systematic TRUS-guided biopsy is low. In these patients, PSAD predicts prostate cancer mortality and provides additional value to other clinical variables. PSAD-based stratification can be used to guide follow-up strategy.
评估在经直肠超声(TRUS)引导下进行的系统性前列腺穿刺活检结果为良性后,前列腺特异性抗原(PSA)密度(PSAD)与前列腺癌死亡率之间的关联。
这项回顾性研究使用了1996年至2020年间收集的芬兰前列腺癌筛查随机研究(FinRSPC)的数据。我们确定了年龄在55 - 71岁之间、随机分配至筛查组、PSA≥4.0 ng/mL且系统性TRUS引导下穿刺活检结果为良性的男性。通过竞争风险函数对以0.15 ng/mL/cm的PSAD为界分层的男性的累积前列腺癌死亡率进行建模。使用c统计量和似然比检验比较PSAD、PSA以及基础变量(穿刺活检时的年龄、直肠指检结果、社会经济状况、5α-还原酶抑制剂使用情况、家族史和Charlson合并症指数(CCI))预测前列腺癌死亡的能力。
在排除了10例穿刺活检后2年内无PSA数据的男性以及65例无前列腺体积数据的男性后,2276名男性符合纳入本研究的条件。在中位(四分位间距)17.4(13.2 - 20.9)年的随访期间,共有50名男性死于前列腺癌,1028名死于其他原因。PSAD<0.15 ng/mL/cm的男性的累积前列腺癌死亡率显著低于PSAD≥0.15 ng/mL/cm的男性:15年时分别为0.5%(95%置信区间[CI] 0.2% - 1.1%)和2.0%(95% CI 1.2% - 3.1%)(Grey检验,P = 0.001)。由PSAD、PSA和基础变量组成的模型预测前列腺癌死亡率(c统计量0.781)显著优于仅由基础变量组成的模型(c统计量0.737;似然比检验,P = 0.003)或由基础变量和PSA组成的模型(c统计量0.765;似然比检验,P = 0.039)。
经系统性TRUS引导下穿刺活检结果为良性后的前列腺癌死亡率较低。在这些患者中,PSAD可预测前列腺癌死亡率,并为其他临床变量提供附加价值。基于PSAD的分层可用于指导随访策略。