Marks Lianna J, Ritter Victor, Agrusa Jennifer E, Kamdar Kala Y, Rivers Julie, Gardner Rebecca, Ehrhardt Matthew J, Devine Kaitlin J, Phillips Charles A, Reilly Anne, August Keith, Weinstein Joanna, Satwani Prakash, Forlenza Christopher J, Smith Christine Moore, Greer Chelsee, Afify Zeinab, Lin Carol H, Belsky Jennifer A, Ding Hilda, Hoogstra David, Toner Keri, Link Michael P, Schultz Liora M, Lowe Eric J, Aftandilian Catherine
Division of Pediatric Hematology, Oncology, Stem Cell Transplantation and Regenerative Medicine, Department of Pediatrics, Stanford University School of Medicine, Stanford, CA.
Biomedical Informatics Research Division, Department of Medicine, Stanford University School of Medicine, Stanford, CA.
Blood Adv. 2025 Mar 25;9(6):1356-1365. doi: 10.1182/bloodadvances.2024014745.
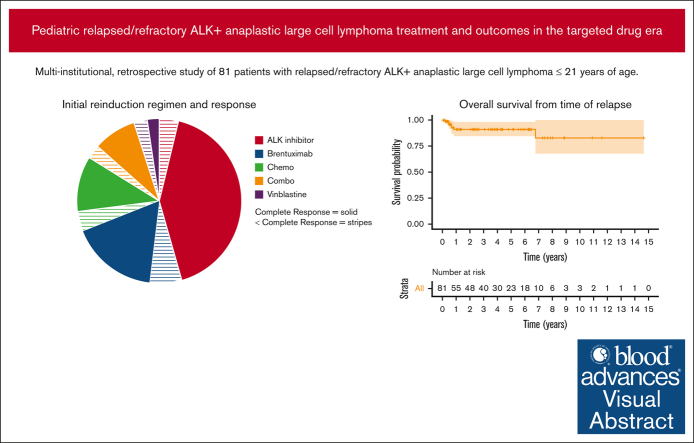
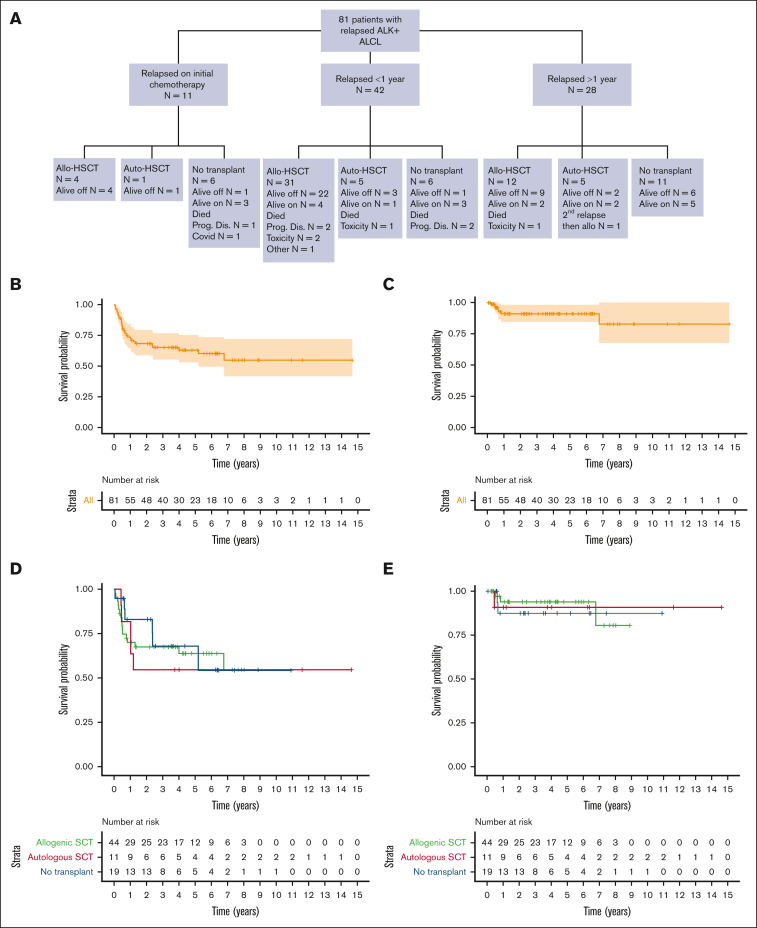
Treatment options for patients with relapsed or refractory (R/R) anaplastic large cell lymphoma (ALCL) have increased in the era of targeted therapies such as brentuximab vedotin (BV) and anaplastic lymphoma kinase (ALK) inhibitors. However, there is no standard treatment and published data evaluating their use are limited. The goal of this retrospective study was to describe current real-world treatment and outcomes of pediatric, adolescent, and young adult patients with R/R ALK-positive ALCL. We conducted a retrospective, multi-institutional study identifying 81 patients with R/R ALK-positive ALCL aged ≤21 years at initial diagnosis treated between 2011 and 2022 across 18 institutions. Median time from diagnosis to relapse was 8.9 months (range, 2.6-131.9). Initial reinduction regimens included ALK-inhibitor monotherapy (n = 37, 46%), BV monotherapy (n = 19, 23%), chemotherapy without targeted therapy (n = 12, 15%), chemotherapy with targeted therapy (n = 9, 11%), or vinblastine monotherapy (n = 4, 5%), with 83% of patients achieving a complete response to initial reinduction regimen. Fifty-eight patients received a hematopoietic stem cell transplant (HSCT), 11 autologous and 48 allogeneic, with 1 receiving both. Duration of treatment for patients receiving BV or the ALK-inhibitor crizotinib (CZ) varied widely (BV, 1-11 years; CZ, 2-10 years). Five-year event-free survival was 63% (95% confidence interval [CI], 53-75) and 5-year overall survival was 91% (95% CI, 84-98). This is, to our knowledge, the largest collection of patients with R/R ALK-positive ALCL treated in the era of targeted therapy. Patients achieved excellent responses to ALK-inhibitor or BV monotherapy, but questions remain about duration of therapy and role of HSCT.
在诸如本妥昔单抗(BV)和间变性淋巴瘤激酶(ALK)抑制剂等靶向治疗时代,复发或难治性(R/R)间变性大细胞淋巴瘤(ALCL)患者的治疗选择有所增加。然而,尚无标准治疗方案,且评估其使用情况的已发表数据有限。这项回顾性研究的目的是描述儿科、青少年和年轻成人R/R ALK阳性ALCL患者当前的实际治疗情况和结局。我们开展了一项回顾性、多机构研究,确定了2011年至2022年期间在18家机构接受治疗的81例初诊时年龄≤21岁的R/R ALK阳性ALCL患者。从诊断到复发的中位时间为8.9个月(范围为2.6 - 131.9个月)。初始再诱导方案包括ALK抑制剂单药治疗(n = 37,46%)、BV单药治疗(n = 19,23%)、无靶向治疗的化疗(n = 12,15%)、有靶向治疗的化疗(n = 9,11%)或长春花碱单药治疗(n = 4,5%),83%的患者对初始再诱导方案达到完全缓解。58例患者接受了造血干细胞移植(HSCT),11例自体移植,48例异体移植,1例接受了两种移植。接受BV或ALK抑制剂克唑替尼(CZ)治疗的患者治疗持续时间差异很大(BV为1 - 11年;CZ为2 - 10年)。5年无事件生存率为63%(95%置信区间[CI],53 - 75),5年总生存率为91%(95% CI,84 - 98)。据我们所知,这是靶向治疗时代接受治疗的R/R ALK阳性ALCL患者的最大病例系列。患者对ALK抑制剂或BV单药治疗反应良好,但关于治疗持续时间和HSCT的作用仍存在疑问。