Baritello Omar, Taxis Theo, Stein Hanna, Luizink-Dogan Machteld, Völler Heinz, Salzwedel Annett
Department of Rehabilitation Medicine, Faculty of Health Sciences Brandenburg, University of Potsdam, Potsdam, Germany.
Department of Rehabilitation Medicine, Faculty of Health Sciences Brandenburg, University of Potsdam, Potsdam, Germany
BMJ Open. 2025 Jan 21;15(1):e083733. doi: 10.1136/bmjopen-2023-083733.
Multicomponent rehabilitation (MR) could restore functioning in elderly patients after hospitalisation, even beyond geriatrics, but specific evidence seems lacking. This review mapped the evidence on MR in elderly patients following hospitalisation for age-related conditions regarding functioning-related outcomes.
Scoping review.
PubMed, Cochrane Library, International Clinical Trials Registry Platform and ClinicalTrials.gov (searched through 24 June 2024).
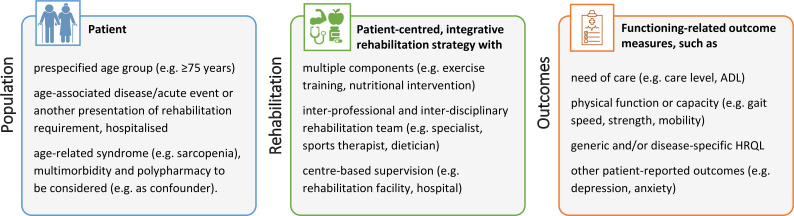
We included randomised controlled trials (RCT) and controlled cohort studies (CCS) comparing centre-based MR with usual care (medical care excluding exercise training) in patients ≥75 years, hospitalised for age-related cardiac, neurological, oncological and orthopaedic diseases. MR was defined as exercise training and at least one additional component (eg, nutritional counselling), starting within 3 months after hospital discharge. RCTs and CCS were included from inception, without language restriction. Care dependency, physical function, health-related quality of life (HRQL) and activities of daily living (ADL) after ≥6 months follow-up were the outcomes of interest.
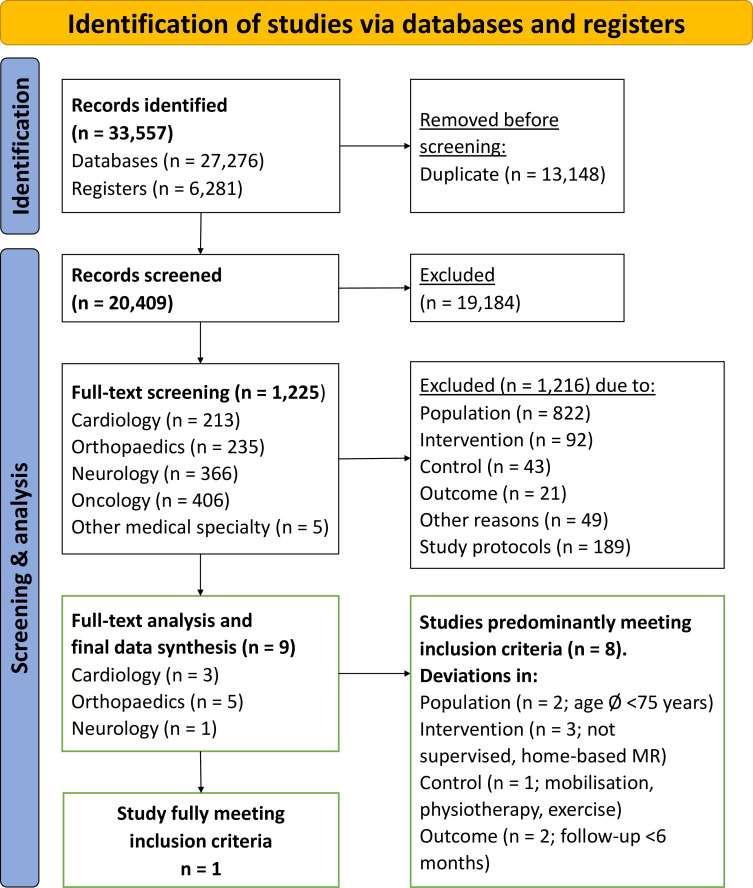
Four reviewers independently screened titles, abstracts and full texts for inclusion and extracted data. MR components and the typology of outcome assessments used were mapped at the final data synthesis level.
Out of 20 409 records, nine studies were investigated in the final data synthesis. Throughout these studies, disease education was the most frequent MR component besides exercise training, while physical function, HRQL and ADL were commonly assessed outcomes. One RCT (cardiac rehabilitation, 80±0.3 years, MR/usual care n=24/23) fully met the inclusion criteria and reported improvements in physical function (2 months) and in HRQL (2, 8, 14 months post intervention) in MR patients.
Evidence on MR regarding functioning-related outcomes in ≥75-year-old patients is sparse beyond geriatrics. There is an essential need for studies investigating the capabilities of MR in this growing and under-represented patient population.
多组分康复(MR)可以恢复老年患者(甚至超出老年医学范畴)住院后的功能,但似乎缺乏具体证据。本综述梳理了老年患者因年龄相关疾病住院后,关于与功能相关结局的MR证据。
范围综述。
PubMed、Cochrane图书馆、国际临床试验注册平台和ClinicalTrials.gov(检索至2024年6月24日)。
我们纳入了随机对照试验(RCT)和对照队列研究(CCS),这些研究比较了年龄≥75岁、因年龄相关的心脏、神经、肿瘤和骨科疾病住院的患者中,基于中心的MR与常规护理(不包括运动训练的医疗护理)。MR被定义为运动训练和至少一项其他组分(如营养咨询),在出院后3个月内开始。从研究开始就纳入RCT和CCS,无语言限制。随访≥6个月后的护理依赖、身体功能、健康相关生活质量(HRQL)和日常生活活动(ADL)是感兴趣的结局。
四名评审员独立筛选标题、摘要和全文以确定纳入情况并提取数据。在最终数据综合阶段梳理了MR组分和所使用的结局评估类型。
在20409条记录中,最终数据综合纳入了9项研究。在这些研究中,除运动训练外,疾病教育是最常见的MR组分,而身体功能、HRQL和ADL是常用的评估结局。一项RCT(心脏康复,80±0.3岁,MR/常规护理n = 24/23)完全符合纳入标准,并报告MR患者的身体功能(2个月)和HRQL(干预后2、8、14个月)有所改善。
除老年医学范畴外,关于≥75岁患者与功能相关结局的MR证据稀少。迫切需要开展研究,调查MR在这一不断增长且代表性不足的患者群体中的作用。