Cotton Antoinette, Salerno Pedro Rvo, Deo Salil V, Virani Salim S, Nasir Khurram, Neeland Ian, Rajagopalan Sanjay, Sattar Naveed, Al-Kindi Sadeer, Elgudin Yakov E
Case Western Reserve University School of Medicine, Cleveland, USA.
Case Western Reserve University School of Medicine, Cleveland, USA; Harrington Heart and Vascular Institute, University Hospitals, Cleveland, USA.
Am J Med Sci. 2025 Apr;369(4):491-497. doi: 10.1016/j.amjms.2025.01.007. Epub 2025 Jan 21.
The American Heart Association recently defined cardio-kidney-metabolic (CKM) syndrome as the intersection between metabolic, renal, and cardiovascular disease. Understanding the contemporary estimates of CKM related mortality in the US is essential for developing targeted public interventions.
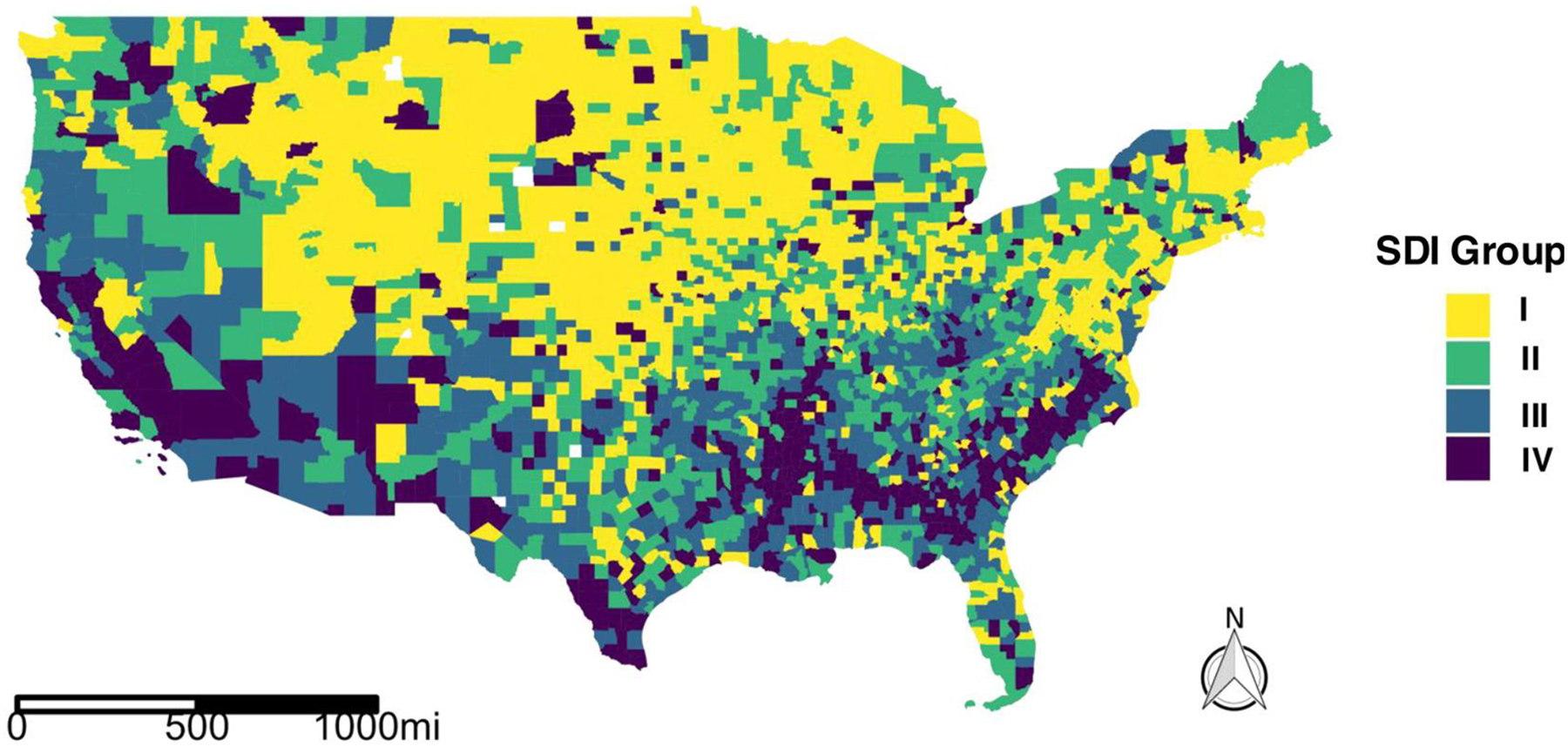
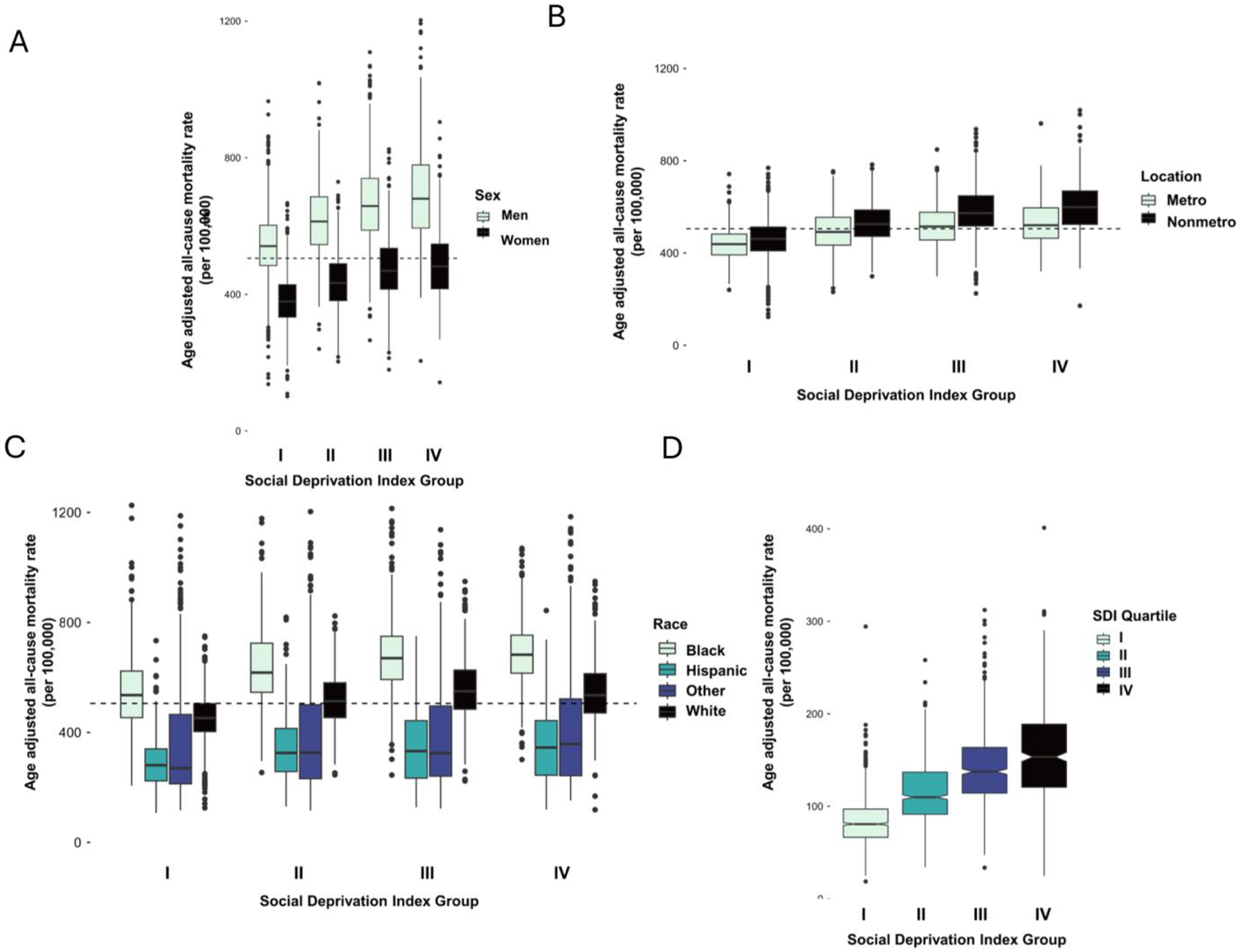
We analyzed state-level and county-level CKM-associated all-cause mortality data (2010-2019) from the CDC Wide-ranging Online Data for Epidemiologic Research (WONDER). Median and interquartile (IQR) age-adjusted mortality rates (aaMR) per 100,000 were reported and linked with a multi-component metric for social deprivation: the Social Deprivation Index (SDI: range 0 - 100) grouped as: I: 0 - 25, II: 26 - 50, III: 51 - 75, and IV: 75 - 100. We fit pairwise comparisons between SDI groups and evaluated aaMR stratified by sex, race, and location.
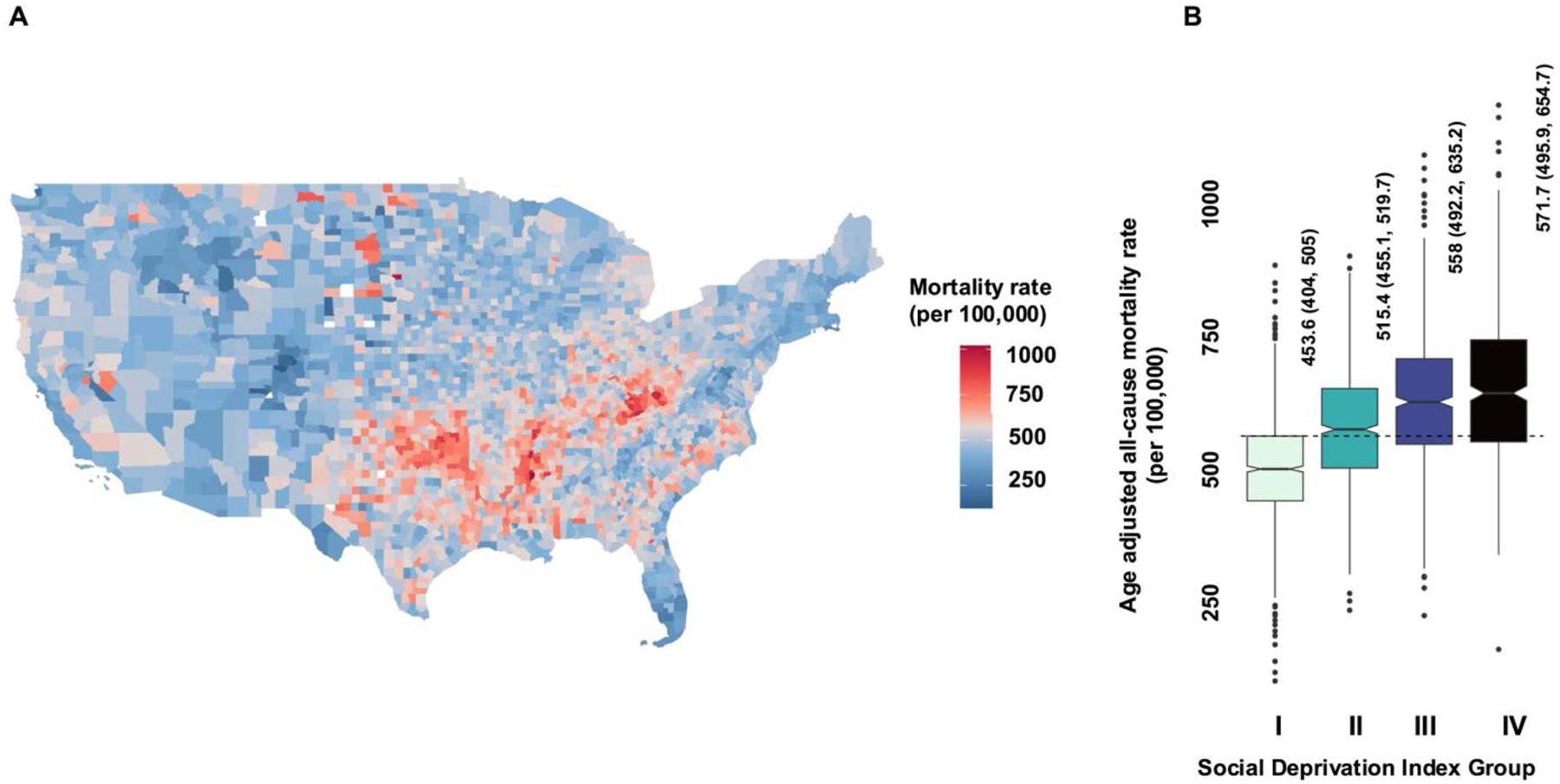
In 3101 counties, pooled aaMR was 505 (441-579). Oklahoma (643) and Massachusetts (364) had the highest and lowest values. aaMR increased across SDI groups [I: 454(404, 505), IV: 572(IQR: 495.9, 654.7); p < 0.001]. Men had higher rates [602 (526, 687)] than women [427 (368, 491)]. Metropolitan [476 (419, 542)] had lower rates than non-metropolitan counties [521 (454, 596)]. Non-Hispanic Black [637 (545, 731)] had higher rates than non-Hispanic White residents [497 (437, 570]. CKM associated aaMR remained reasonably constant between 2010 and 2019 (Mann Kendall test for trend p-value = 0.99).
In the US, CKM mortality disproportionately affects more socially deprived counties. Inability to reduce CKM mortality rates over the study period highlights the need for targeted policy interventions to curb the ongoing high burden.
美国心脏协会最近将心脏-肾脏-代谢(CKM)综合征定义为代谢、肾脏和心血管疾病的交叉点。了解美国CKM相关死亡率的当代估计值对于制定有针对性的公共干预措施至关重要。
我们分析了美国疾病控制与预防中心(CDC)的广泛在线流行病学研究数据(WONDER)中2010年至2019年州级和县级与CKM相关的全因死亡率数据。报告了每10万人的年龄调整后死亡率中位数和四分位间距(IQR),并与社会剥夺的多成分指标相关联:社会剥夺指数(SDI:范围0 - 100)分为:I:0 - 25,II:26 - 50,III:51 - 75,IV:75 - 100。我们对SDI组之间进行了成对比较,并评估了按性别、种族和地理位置分层的年龄调整后死亡率。
在3101个县中,汇总的年龄调整后死亡率为505(441 - 579)。俄克拉荷马州(643)和马萨诸塞州(364)的值最高和最低。年龄调整后死亡率在SDI组中呈上升趋势[I组:454(404, 505),IV组:572(IQR:495.9, 654.7);p < 0.001]。男性的死亡率[602(526, 687)]高于女性[427(368, 491)]。大城市县[476(419, 542)]的死亡率低于非大城市县[521(454, 596)]。非西班牙裔黑人[637(545, 731)]的死亡率高于非西班牙裔白人居民[497(437, 570)]。2010年至2019年期间,与CKM相关的年龄调整后死亡率保持相对稳定(Mann Kendall趋势检验p值 = 0.99)。
在美国,CKM死亡率对社会剥夺程度较高的县影响尤为严重。在研究期间未能降低CKM死亡率凸显了需要采取有针对性的政策干预措施来遏制持续的高负担。